
Commentary
By Natasha Benn
Evelyn, a 67-year-old woman, walks into a doctor’s office hoping to receive treatment and pain management strategies for her ongoing hip osteoarthritis. However, what she hears instead are these comments: “you need a walker”, “you’re going to fall and break your hip”, and “someone of your age needs to be careful”. As a result, Evelyn walks out of the doctor’s office feeling discouraged and afraid of falling. Fear-inducing conversations regarding falls occur every day across Canada, not just in health care settings, but in media and within social circles. These conversations can produce a Fear of Falling (FOF) effect. It is also common, as 20.8-85% of people over the age of 65 reporting a FOF (1). A review also found that a FOF is an independent predictor of a significantly reduced quality of life (2). FOF can be described in two ways (2): (a) The person has fearful anticipation of a future fall, and (b) the person has lost their confidence in themselves during various activities of daily living. FOF typically presents as a cyclical process (Figure 1) (3):
- First, a FOF develops through a previous fall and/or through anxiety-driven conversations regarding the negative consequences of falls.
- After a FOF develops, the person will decrease their activity levels.
- Inactivity will subsequently decrease their strength, coordination, and balance.
- Consequently, this will directly increase their risk of falls and exacerbate their FOF.
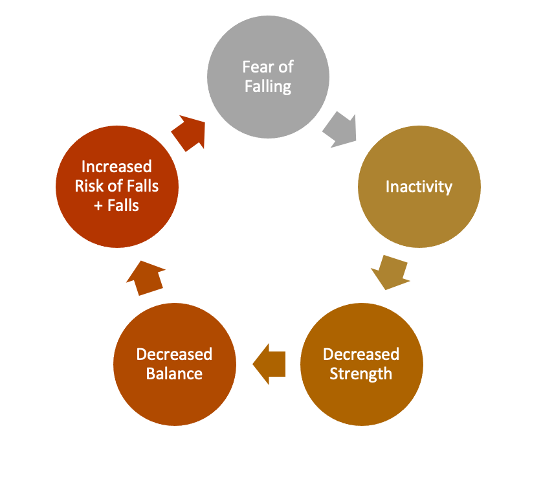
Figure 1. Cycle of Fear of Falling
The main questions that come from this cycle are: how do we prevent FOF from occurring, and how do we stop the cycle once it begins? As a practicing physiotherapy clinician in Canada, I would argue that one of the most significant ways health care professionals can prevent FOF from occurring and developing, is by changing our communication approach with people at risk of falling. It is important to educate people on the risk of falls using a motivational approach. Instead of inducing fear, it is important to make the patient excited to engage in a falls prevention program, where impactful improvements can be made to prevent or stop the FOF cycle (4). Focusing on a solution that emphasizes the improvements in their daily life and independence will enable them to have hope and motivation to start or continue with therapy.
There are several reasons why focusing on fear-inducing conversations about falls will not help populations at risk; two of the reasons include (5,6): (a) The person sees falling as a sign of aging and loss of independence; these individuals are in denial of their risk of falling and will not seek therapy due to social identity, and (b) the person develops a FOF, and it occurs in 25% of people who have a history of falls (7) (Table 1). People can experience both reasons at the same time and both can lead to fear-avoidance behaviour, characterized by avoiding activities in their daily lives, which makes them less likely to seek preventative programs.
“It is important to educate people on the risk of falls using a motivational approach. Instead of inducing fear, it is important to make the patient excited to engage in a falls prevention program, where impactful improvements can be made to prevent or stop the FOF cycle (4).”
In the first example, they are determined to maintain their active independence and are worried about the social ramifications of being considered old and frail due to falls being a symbol of aging in society (5). In turn, they are less likely to seek preventative health therapies for falls, like balance therapy (5). Independence is a major concern for all, whether a person believes they are at risk for falls or not. Therefore, it is important communicate to individuals that preventative therapies, like balance therapy, will help maintain or improve independence more successfully for these populations (6). Another interesting finding from a study was that older individuals generally dislike health promotion messages targeted at older adults (6). The older adults in this study described that they are motivated to exercise by psychosocial factors and not for the older adult health benefits (6). Media and conversations stating, “stay active, stay independent,” may help this group to seek preventative therapies, as it does not discuss their fall risk or that they are any less independent currently, but need to seek preventative therapy to maintain independence (5).
In the second example, the people are caught in the FOF cycle, where fall-awareness media campaigns that exacerbate their fear are detrimental to their success. Research has shown that individuals with positive perceptions towards aging are more likely to access preventative health care, suggesting that reinforcement of positive aging could facilitate further preventative therapy uptake (5). A suggestion by a qualitative paper emphasizes focusing on independence and “staying healthy” messages (5). This study showed three messages to older adults, one focusing on falls, the other on health, and the last on independence (5). In interviews, all participants discussed disliking the falls prevention message, and some viewed it as “detrimental” (5). Instead, participants liked the messages containing a focus on positive improvements in balance, health, and independence (5). Independence is linked with being able to stay in one’s own home, pride, reducing liability on others, and perception of self-worth in older adults (5). Interestingly, a couple of participants noted that they view a loss of independence as inevitable with age and would prefer statements like, “be the best that you can be,” (5). This kind of statement acknowledges the decline in physical function with age, but that there is always room for improvement with therapy.
| Table 1: Recommendations for communication, per Hughes and colleagues (2008) (5) | |
| Patient Perception | Response |
| Currently has a FOF | – A focus on the improvements and increased independence that one will get with therapy
– Ensure in your education about the risk of falls that therapy can improve their balance and reduce the risk. – Emphasize a positive aging image. “Because of “x” factors, you are at an increased risk of falling which can result in injuries. However, through therapy, you will be able to improve your balance, increase your independence, and reduce your risk of falls.” |
| Believes falls are a sign of aging and worried about the psychosocial impact | – A focus on maintenance of their independence.
– Potentially could add the psychosocial benefits as well if suggesting a group therapy. “By taking steps to improve your balance and function now we can mitigate those risks and maintain your current level of independence for as long as possible.” |
| Believes falls and reduced balance are inevitable with aging | – A focus on improving their balance and independence as much as the person possibly can to enhance their daily activities
“I understand that you believe you will not get back to your level of functioning from when you were in your 20s, however therapy can significantly improve your current day to day tasks.” |
Currently, the best way to measure a person’s FOF is by measuring their balance self-efficacy, which is the level of confidence an individual has in performing daily activities without losing their own balance (8). A common measure for balance self-efficacy is the Activities-specific Balance and Confidence scale (ABC Scale), which assesses a person’s balance self-efficacy and monitors for change over time with therapy.
The importance of assessing and treating FOF can be seen in the literature. A study by Franchignoni et al (2005) demonstrated in patients with Parkinson’s Disease that balance and postural control were directly related to the complex interactions between a FOF, motor impairment, and functional abilities (9). In a study by Danks et al (2016), they found a significant correlation between walking capacity and balance self-efficacy (10). Another study found similar findings for people with Parkinson’s Disease, showing that balance self-efficacy accounted for 17% of the variability of functional walking capacity (11). Finally, a study by Lajoie et al (2004) demonstrated that an accurate prediction of falls risk can be achieved using only a physical balance test (Berg Balance Scale) and the ABC Scale, with 89% sensitivity and 96% specificity, indicating a high accuracy (4). These studies demonstrate the importance and the relationship between balance self-efficacy and physical outcomes, and the potential impact of reducing FOF to improve participation in activities, functional outcomes, and fall risk (12).
Recommendations for Therapies:
- Local physiotherapist
- Canadian Physical Activity Guidelines (13)
- Tai Chi (14)
- Balance exercises in the pool (15)
- Walking with appropriate gait aid
The first step that I propose to reduce the prevalence of FOF is for health care professionals and media campaigns to focus communication and messaging on balance and independence to promote falls-prevention therapies. Using this style of communication is hypothesized in the literature to reduce FOF, and to enhance the public’s motivation to participate in preventative balance therapies (5).
Acknowledgements
Featured illustration by tegh 93 from Pexels.
To refer to this article, it can be cited as:
Benn N. The Power of Words: How to Talk About Fall Risk. rehabINK. 2022:13. Available from: https://rehabinkmag.com
References
- Scheffer AC, Schuurmans MJ, van Dijk N, van der Hooft T, de Rooij SE. Fear of falling: measurement strategy, prevalence, risk factors and consequences among older persons. Age Ageing. 2008 Jan;37(1):19–24.
- Schoene D, Heller C, Aung YN, Sieber CC, Kemmler W, Freiberger E. A systematic review on the influence of fear of falling on quality of life in older people: is there a role for falls? Clin Interv Aging. 2019 Apr;Volume 14:701–19.
- Cumming RG, Salkeld G, Thomas M, Szonyi G. Prospective Study of the Impact of Fear of Falling on Activities of Daily Living, SF-36 Scores, and Nursing Home Admission. J Gerontol A Biol Sci Med Sci. 2000 May 1;55(5):M299–305.
- Lajoie Y, Gallagher SP. Predicting falls within the elderly community: comparison of postural sway, reaction time, the Berg balance scale and the Activities-specific Balance Confidence (ABC) scale for comparing fallers and non-fallers. Arch Gerontol Geriatr. 2004 Jan;38(1):11–26.
- Hughes K, van Beurden E, Eakin EG, Barnett LM, Patterson E, Backhouse J, et al. Older Persons’ Perception of Risk of Falling: Implications for Fall-Prevention Campaigns. Am J Public Health. 2008 Feb;98(2):351–7.
- Yardley L, Bishop FL, Beyer N, Hauer K, Kempen GIJM, Piot-Ziegler C, et al. Older People’s Views of Falls-Prevention Interventions in Six European Countries. The Gerontologist. 2006 Oct;46(5):650–60.
- Nevitt MC. Risk Factors for Recurrent Nonsyncopal Falls: A Prospective Study. JAMA. 1989 May 12;261(18):2663.
- Powell LE, Myers AM. The Activities-specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci. 1995 Jan 1;50A(1):M28–34.
- Franchignoni F, Martignoni E, Ferriero G, Pasetti C. Balance and fear of falling in Parkinson’s disease. Parkinsonism Relat Disord. 2005 Nov;11(7):427–33.
- Danks KA, Pohlig RT, Roos M, Wright TR, Reisman DS. Relationship Between Walking Capacity, Biopsychosocial Factors, Self-efficacy, and Walking Activity in Persons Poststroke. J Neurol Phys Ther. 2016 Oct;40(4):232–8.
- Mak MKY, Pang MYC. Balance self-efficacy determines walking capacity in people with Parkinson’s disease. Mov Disord. 2008 Oct 15;23(13):1936–9.
- Kostanjsek N. Use of The International Classification of Functioning, Disability and Health (ICF) as a conceptual framework and common language for disability statistics and health information systems. BMC Public Health. 2011;11(Suppl 4):S3.
- Canadian Society for Exercise Physiology (CSEP). Canadian 24-Hour Movement Guidelines: An Integration of Physical Activity, Sedentary Behaviour, and Sleep [Internet]. CSEP Guidelines. 2022 [cited 2022 Apr 28]. Available from: https://csepguidelines.ca/
- Hakim RM, DiCicco J, Burke J, Hoy T, Roberts E. Differences in Balance Related Measures Among Older Adults Participating in Tai Chi, Structured Exercise, or No Exercise: J Geriatr Phys Ther. 2004 Apr;27(1):13–7.
- Peter Douris, Southard V, Varga, C, Schauss W, Gennaro C, Reiss A. The Effect of Land and Aquatic Exercise on Balance Scores in Older Adults. Journal of Geriatric Physical Therapy. 2003;26(1):3–6.
