Since COVID-19 response measures first began in Canada in March, life as we know it has been constantly changing. Everyone was encouraged to stay home, and many people calmed their nerves by keeping up with the news and staying informed. What became prominent, however, was the sheer abundance of factual and non-factual information. The rehabINK Podcast team’s desire to decrease the gap between scientists and the community came into fruition as the COVID-19 mini-series.
COVID-19 Mini-Series: A Student Engagement Initiative
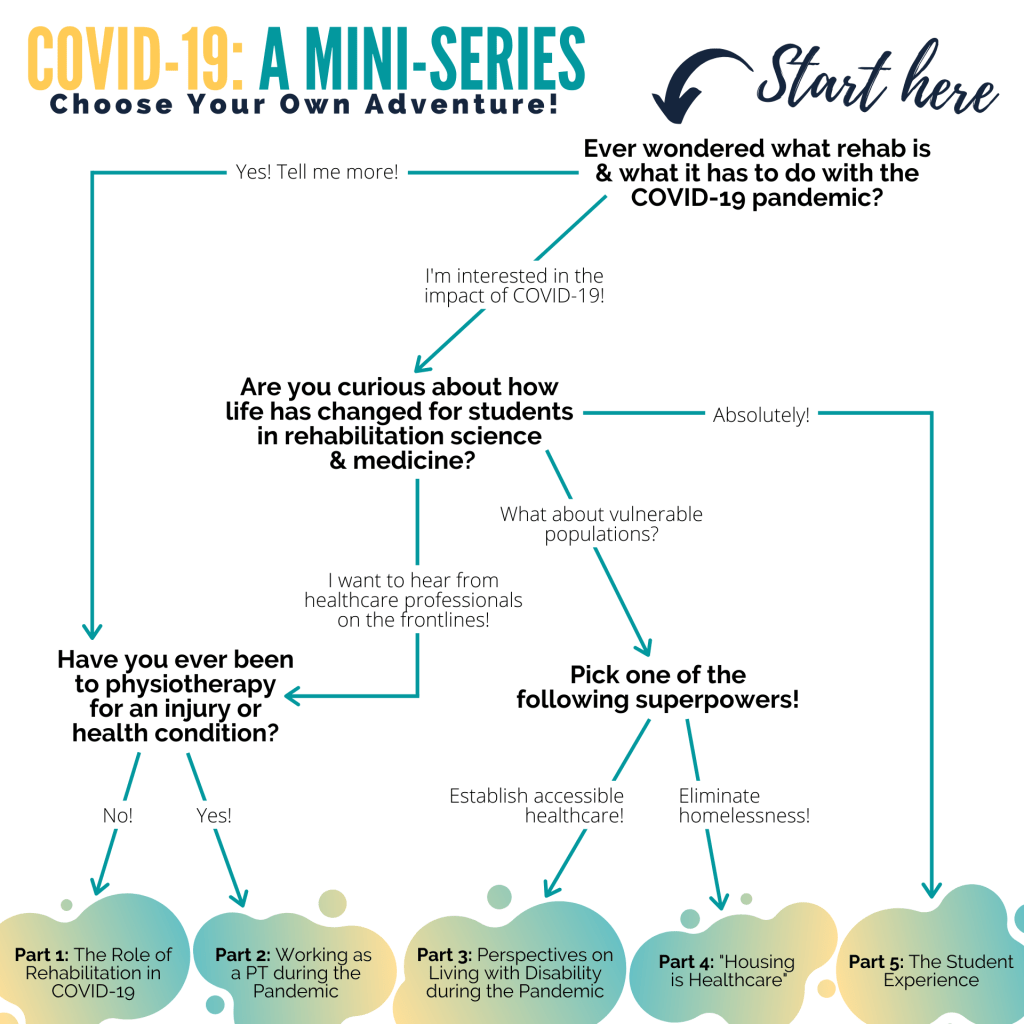
Given the new realities of social distancing and heightened risk of illness, the mini-series aimed to discuss how the pandemic is changing rehabilitation research, clinical care, and the graduate student experience. We wanted to create episodes which encourage meaningful conversations, explore innovative solutions, and contribute towards a greater understanding of the pandemic.

Part 1: The Role of Rehabilitation in COVID-19
In the first installment of the Mini-Series, we introduced the importance of rehabilitation for COVID-19 recovery. For many, the virus brings to mind immediate and acute dangers related to survival, but long-term recovery trajectories are becoming of increased importance. The first episode introduces the perspectives of those clinicians involved in the next stage of COVID-19 care: rehabilitation.
Dr. Larry Robinson, Siobhan Donaghy and Jennifer Shaffer discuss their learnings:
- Change management is essential. Organizational efforts were set in motion to receive COVID-19 patients. Rehabilitation facilities and intervention plans were adjusted to discharge patients early. Staff training was set-up to provide education on the use of personal protective equipment, and different channels were opened for the healthcare team to share their concerns.
- Healthcare flexibility and resourcefulness. Interprofessional team members learned new skills outside of their typical responsibilities to maximize patient engagement while maintaining physical distancing (e.g., physiotherapist assisted with self-care). Everyone quickly learned which items can and cannot be safely disinfected. Common items in the room were repurposed for use in assessment and treatment.
- Psychosocial support is needed. Staff and patients were mentally exhausted by the fears of infection and the need to maintain social isolation. To relieve the fatigue, hospital administration arranged for more mental health resources. For example, volunteers visited patients individually and connected them with their families through video calls. Staff also organized celebrations for birthdays and discharge, which did wonders to maintain morale for everyone.
Part 2: Working as a PT during the pandemic
In the second episode, we take a deeper dive into the experiences of rehabilitation healthcare providers working during COVID-19. We hear from Michelle Legasto, a PhD student and physiotherapist. When a call for skilled healthcare professionals was released, Michelle volunteered to be redeployed to a long-term care home. Michelle shares her learnings from working with vulnerable and COVID-19 patients during the pandemic.
- Social distancing and isolation. For the first few months of the pandemic, Michelle would only leave home for essential trips. She was worried about being an asymptomatic carrier of COVID-19 who would infect others in the community. Michelle declined invitations to meet with family and friends and opted to take her regular walks during the quiet hours of the night.
- Mental health support for healthcare workers. Michelle praises Sunnybrook and their management for arranging mental health support for staff working with COVID-19 patients. A dedicated contact would regularly check-in with Michelle on how she was doing and offer support. Sunnybrook had also formed a peer support group, where she reported great relief in being able to share her experiences with others going through the same things.
- Communication barriers and masks. At work, everyone was wearing multiple layers of personal protective equipment (PPE), including masks and face shields. The amount of PPE acted as a barrier for the virus and communication with others. Visual cues play an important role in understanding speech and this is especially important for people who were hard of hearing. Extensive PPE also made it challenging for her and patients to figure out who they were speaking to when you can only see their eyes. Michelle spoke about writing her name on the face shield and stickers would be a faster way to identify others.
Part 3: Perspectives on Living with Disability during the Pandemic
For the third episode of the COVID-19 series, we take a closer look at the other side of healthcare: people with lived experiences. Dr. Susan Jaglal and John Shepherd from the University of Toronto discuss the perspectives of people living with disability.
- Staying informed and the world. New information shapes how we interact with the world. Earlier on in the pandemic, people using wheelchairs would follow a strict regimen for sanitizing their hands and wheelchairs when they returned home. We now understand that virus transmission is unlikely from contact surfaces. The lessons we learned from then have taught us good hand hygiene and physical distancing, which likely helped to reduce the number of individuals contracting the flu this year.
- Changes in healthcare access. There are currently additional restrictions to access healthcare and necessary supports for daily living. Many people with disabilities spent the first few months figuring out how to live in this new normal. On the flip side, people are now becoming more comfortable with using technology. As a result, more people can get prescription refills and medical advice from home.
- Virtual social events. People are staying home more often than before, and this is especially the case for people living with disabilities. Virtual access has offered more opportunities to engage in social activities and maintain social connections.
Part 4: Housing is Healthcare
On the penultimate episode, we delve into the impact of COVID-19 and social determinants of health on health outcomes. We speak with Dr. Naheed Dosani about homelessness and structural vulnerability, systemic inequities, and advocacy in healthcare.
- Homelessness is making sick people sicker. Housing facilities are reducing their hours, restricting occupants to maintain social distancing, and temporarily closing because of COVID-19. Many people living with homelessness are opting to stay outside and delaying access to healthcare due to the fear of contracting COVID-19. Limited housing and inadequate funding for social supports have resulted in emotional distress and faster progression of disease for people living with homelessness.
- Privilege and equality. For many who are living in poverty, structural access makes it practically impossible to access new technologies such as the COVID alert mobile app and virtual care. These technologies require the latest phone, the latest software, and internet access, which are only available to individuals with housing and disposable income.
- Be an advocate for social justice. We live in a society where we are constantly on the go. Engagement becomes another item that we will eventually get to in our ever-growing to-do lists. We urge our audience to reflect on the causes that matters to them. Take the time listen and learn from those with lived experiences to better inform yourself and others. Act by sharing your power and your privilege. Amplify the voices of those with lived experiences.
Part 5: The Student Experience
On the final episode of the COVID-19 series, we invited students from the Temerty Faculty of Medicine at the University of Toronto to share their experiences as a graduate student in clinical and research programs.
- Delays in education. In-person labs and internships were delayed for students across different clinical programs. Students were concerned with their ability to learn and apply their skills in the clinic. For research students, in-person data collection was practically impossible. While some students were able to transition to collecting data online, many students were unable to do so. These adjustments meant that students were faced with the need to change their research and delay graduation.
- Blanket approach to student needs. The pandemic did not affect everyone equally, especially students. Regardless, a blanket response to COVID-19 was used to address student needs. Universities aimed to keep students in-the-know by hosting townhalls and providing regular updates. They also enforced contact tracing and established mental health supports. Instructors did their best to adapt educational materials for online learning and checked-in regularly on students. However, it is unclear how well students are learning and how effective these strategies were in supporting such a diverse student population.
- Virtual care. Virtual care may be becoming the standard practice for service delivery. Aspiring healthcare providers may be expected to be familiar with virtual care. Further, accessibility concerns in the future may revolve around internet access and the need for safe and private spaces.
- Silver linings. COVID-19 has helped us better appreciate the little things in life such as spending time with family and being outdoors. We are trying to take better care of ourselves by eating healthier, engaging in physical exercise, practicing mindfulness, and maintaining social connections. Many students said that they have gained the much-needed time to reflect and slow down, and learned a little bit more about themselves.
Summary: The learnings from a global pandemic
COVID-19 has taught us many lessons in the year 2020:
- It has accelerated the advancements of virtual care and online education.
- It has informed the public on the importance and range of rehabilitation sciences.
- It has served to reduce barriers for some and for others, has increased inequities.
- It has opened dialogue to drive positive change for various social issues.
- It has helped us learn to be comfortable with the unknown.
Conclusion: Rehabilitation and the future
We hope you found the COVID-19 Mini-series insightful. With the second wave of COVID-19 surging, it will be challenging to consider the lasting effects of the pandemic. The need for an equity lens and having marginalized communities on the centre of conversations will be essential during the recovery period of COVID-19.
We can be assured that the rehabilitation community is continuing to make considerable strides towards better supporting patients and their loved ones amidst the storm. Until the storm calms, please continue to celebrate the small successes in your day-to-day life and take care of yourself.
Listen and learn. We welcome the opportunity to amplify the voices of those with lived experiences. Stay connected by following us on social media. Let us know if you have a story you would like to share on the rehabINK podcast. We would love to listen and learn from you!
You can listen to all the podcast episodes here: COVID-19: A Mini-Series
Acknowledgements. We would like to thank our guests for their time and insight; our listeners for your attention and continued interest; as well as our sponsors, the University of Toronto for supporting this initiative. The COVID-19 mini-series is a 5-part podcast supported by the student engagement fund at the University of Toronto.
