Mini Review
By Vanessa S.K. Fan, Riya Shah, Sharon S. Kwan, Anna Krosinski
Approximately 78,000 Ontarians have experienced short or long–term post-COVID-19 conditions (1). Post-COVID-19 conditions can be defined as ‘symptoms persisting or recurring for weeks after acute COVID-19 illness’ (2), which are categorized into physical (e.g. fatigue, pain, insomnia), cognitive (e.g. concentration loss), or psychological impairments (e.g., anxiety, depression) (1). Survivors of COVID-19 (i.e., people diagnosed with COVID-19 who remain alive) with the above impairments likely experience mental and functional needs (3). Mental health conditions can contribute to poor physical, social, and occupational functioning (4-5). People with mental challenges have impaired processing of social cues and functioning (6,7). Depression also impairs cognitive processing (8), memory (9), concentration (10), and energy level (11), resulting in absenteeism and presenteeism (12). People with post-COVID-19 conditions may require rehabilitation, thereby imposing a significant burden on the healthcare system. Menges et al. (2021) found that a significant proportion of survivors develop post-COVID-19 symptoms which require additional healthcare services. In fact, 36% reported further general physician visits, 7% made emergency calls, and 10% of previously hospitalized patients need rehospitalization due to persistent and complicated post-COVID-19 conditions (13). Previous studies found that cognitive behavioural therapy (CBT) is effective in addressing mental and functional needs in populations other than survivors of COVID-19 (14). Thus, we hypothesized that CBT is beneficial in addressing mental and functional needs among survivors with COVID-19.
The National Institute for Health and Care Excellence in the United Kingdom has recommended CBT for patients with the following conditions: depression, generalized anxiety disorder, panic disorder, obsessive-compulsive disorder (OCD) and post-traumatic stress disorder (PTSD) (15). The above conditions are likely to occur in survivors of COVID-19 (1). A meta-analysis by Hofmann et al. demonstrated that CBT significantly improved mental well-being and quality of life across different mental health diagnoses (16). Previous studies found a 5-fold increase in CBT registration for OCD during COVID-19 compared to pre-COVID-19, highlighting the need for psychological support associated with the pandemic (17). Thus, identifying effective interventions that address post-COVID-19 deficits are highly warranted. Here, we took a rapid review approach to examine the evidence of CBT in addressing functional and mental health needs among survivors of COVID-19.
What is CBT?
CBT is a self-directed and structured psychotherapy that aims to alleviate people’s emotional distress by introducing adaptive thoughts and behaviours (18). CBT is a time-limited program, ranging from 6 to 20 sessions (19). CBT can be done online independently or facilitated by registered healthcare professionals1 (19,20) with adequate training with CBT, in person, virtually, one-on-one, or in a group (21). In CBT, people “learn to identify, question and change the thoughts, attitudes and beliefs related to the emotional and behavioural reactions that cause them difficulty” (19). CBT is based on Beck’s Cognitive Model, which suggests that changing behaviours and thoughts can affect our mood, and vice versa (Figure 1). For instance, people with a mental illness often experience negative thoughts on a particular situation (e.g., “When I am not productive at work, I will be worthless”), leading to low mood or unhelpful coping behaviours (e.g. uncontrolled alcohol use). Thus, CBT teaches people to regulate their mood by reframing their cognitive distortions and introducing behaviours that boost their mood (19).
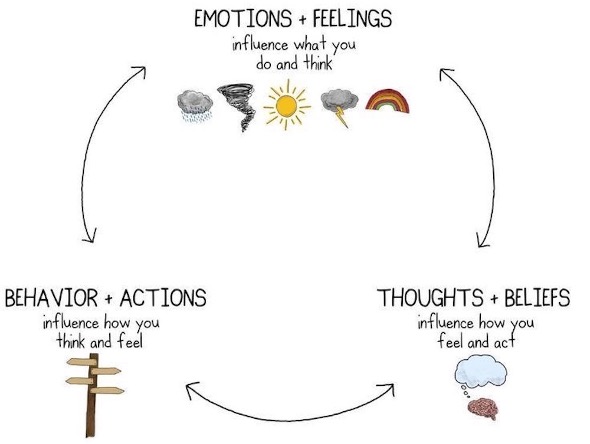
This is a photo of a cycle of “emotions + feelings”, “thoughts + beliefs”, and “behaviours + actions”. “Emotions + feelings” are at the top of the cycle, with the description “influence what you do and think” underneath. Graphic drawings of a cloud, tornado, sun, lightning cloud, and rainbow are below the description. Two sided arrows are between ” emotions + beliefs” and “thoughts + beliefs.” “Thoughts” + beliefs are on the bottom right of the cycle, with the description “influence how you feel and act”. A graphic image of a brain with a thinking cloud is below the description. There is a two sided arrow between “thoughts + beliefs” and “behavior + action.” “Behavior + actions” are on the bottom left side of the cycle. The description “influence how you think and feel,” with a graphic image of a road sign is below. There is a two sided arrow between “behavior + actions” and “emotions + feelings.”
How does CBT Work in Improving Mental Health and Daily Functioning?
CBT improved quality of life by reducing the severity of mental health conditions (e.g., depression, panic disorder, and social anxiety disorder) even one-year post-intervention (23-25). CBT has also effectively promoted occupational and social functioning and quality of life (26-27). Zhang et al. (2016) found that social support, functioning, and quality of life increased significantly among those with mild depression even 1 year after CBT (26). These findings suggest that CBT improves everyday–function in the long-term among individuals with mild depression. Another study found that 41% of particpants, who were seeking employment, found employment after 16 weeks of CBT. Among those who were consistently employed, presenteeism significantly decreased, which correlated with lower negative cognitive styles following CBT, meaning participants were better able to focus at work and accomplish tasks (27). The findings suggest that CBT improves occupational functioning and quality of life among those with major depressive disorder.
What is the Current Evidence of CBT in Addressing Mental Health and Functional Needs Among Survivors of COVID-19?
Four studies were conducted to examine the effectiveness of CBT in addressing insomnia and mental health concerns (i.e., depression, anxiety, PTSD) among patients with COVID-19 (28–31). All studies were from China, with sample sizes varying from 26-252 (28–31). Half of the CBT interventions were delivered in a virtual or hybrid format (28,30).
While 2 studies showed that CBT reduces depression and anxiety symptoms (29,30), 2 other studies support its use in reducing insomnia and PTSD symptoms (28,31). No studies examined the effectiveness of CBT in improving functional outcomes among people with COVID-19 diagnoses.
1. Insomnia
He et al. (2021) tested a simplified version of CBT for insomnia for female survivors of COVID-19 with acute insomnia (i.e., caused by changing environment and stress) or chronic insomnia in a mobile cabin hospital reconstructed hospital from stadium and conference centers (28). The simplified CBT included (i) education on COVID-19, self-protection against COVID-19, and sleep hygiene, (ii) behavioural strategies such as stimulus control and relaxation, and (iii) coping strategies against group separation and building a support system (28). The intervention group reported significant improvements in insomnia severity, shorter time required to falling asleep, and longer sleep time (28). The sleep quality improved in over 80% of the acute insomnia group (n=31) and 70% in the chronic insomnia group (n=35) (28). Fewer medications were used to improve sleep in the acute insomnia group than those in the chronic insomnia group (28).

2. Depressive, anxiety symptoms, and stress
Two studies consistently demonstrated CBT’s effectiveness in reducing depressive and anxiety symptoms among survivors of COVID-19 under isolation in hospitals (29,30), yet the content of the CBT program was slightly different (29,30). In Liu et al.’s study, the cognitive component of CBT aimed to teach participants sleep management skills, help them understand how stress can cause physical symptoms and reduce their irrational thoughts about COVID-19 (29). The behavioural strategies were introduced to help participants regulate their negative emotions through relaxation, mindfulness and meditation (29). Compared to those receiving usual treatments (i.e. control group, n=126), survivors of COVID-19 who received computerized CBT in addition to the routine treatment (n=126), consisting of regular psychological assessment, general psychological support, consultation on overall well-being and disease activity, reported a significant reduction in depressive symptoms, anxiety symptoms, and insomnia after 1-week of computerized CBT and even at the 1-month post-intervention follow-up (29).
Another study by Li et al. demonstrated a greater reduction in anxiety, depression, and stress among those participating in CBT (n=47), compared to those who did not (n=46) (30). Their CBT intervention used cognitive strategies to correct misconceptions about COVID-19 by providing accurate knowledge about COVID-19 and symptom management strategies (30). The behavioural strategies aimed to help participants cope with COVID-19 and included teaching clients about self-protection behaviours (e.g., proper handwashing) and relaxation skills (30). One additional component was encouraging participants to obtain social support from friends and family (30).
While CBT is effective in addressing distress, survivors of COVID-19 with a more extended hospital stay or chronic disease may require more support. Within the CBT group, survivors of COVID-19 with longer hospital stays had lower anxiety, depression, and stress reductions than those with shorter hospital stays (30). Similarly, survivors of COVID-19 with chronic disease had a smaller anxiety reduction after CBT than those without the chronic disease (30). This finding suggests that future research is needed to understand the specific needs among survivors of COVID-19 with lengthy hospitalization or chronic conditions and optimize CBT to support them better.
3. PTSD
A previous study suggests that acute infectious diseases can lead to PTSD (32), which likely puts survivors of COVID-19 at a high risk of having PTSD. The study by Fan et al (2021) tested a CBT-based narrative exposure therapy in reducing PTSD symptoms among survivors of COVID-19 (31). The narrative exposure therapy intended to reduce the impact of PTSD symptoms on daily functioning, which included psychoeducation to normalize negative emotions such as anxiety, helping participants process their emotions, and identifying new hopes through exposure to traumatic memories (31). They found that a CBT-based narrative exposure therapy significantly reduced PTSD symptoms (i.e., re-experiencing traumatic experience, numbing, and hyperarousal) among survivors of COVID-19 after an 8-week narrative exposure therapy session either in virtual or in-person formats (n=56) (31).
“People with post-COVID-19 conditions may require rehabilitation, thereby imposing a significant burden on the healthcare system”
Conclusion
COVID-19 has resulted in a growing population with post-COVID-19 impairments. Poorly managed post-COVID-19 conditions can cause mental and functional needs, increasing rehabilitation demands. This rapid review showed that CBT helps to alleviate anxiety, depression, PTSD symptoms, and insomnia among survivors of COVID-19. Yet, more research is needed to demonstrate the role of CBT in improving function.
Available online resources
| Online resource | Description |
| MindBeacon | Digital iCBT is free for Ontarians. (https://info.mindbeacon.com/btn542) |
| AbilitiCBT | Can be accessed at any time; involves ten structured models that one moves through at their pace and scheduled check-ins with the therapist. (https://ontario.abiliticbt.com/home) |
| Beating the Blues | For individuals with depression or anxiety; weekly eight sessions of reading material and practical coping strategies (https://www.beatingtheblues.co.uk/) |
| Moodym | Five interactive modules that look into one’s feelings, thoughts, stress, and relationships; helps to practice skills to manage symptoms of anxiety or depression. (https://moodgym.com.au/) |
| NHS inform | Mental health self-help guides that utilize CBT techniques; target different areas of mental health, including anxiety, depression, phobias, PTSD, and social anxiety. (https://www.nhsinform.scot/illnesses-and-conditions/mental-health) |
Acknowledgements
Featured image by Fusion Medical Application (Unsplash).
To refer to this article, it can be cited as:
Fan VSK, Shah R, Kwan SS, Krosinski A. Is cognitive behavioural therapy a beneficial rehabilitation strategy to address mental and functional needs among survivors of COVID-19? rehabINK. 2022:13. Available from: https://rehabinkmag.com
References
- Razak F, Katz GM CA et al. Understanding the post COVID-19 condition (long COVID) and the expected burden for Ontario. Science Briefs of the Ontario COVID-19 Science Advisory Table. 2021;2(44).
- Government of Canada. Post COVID-19 condition [Internet]. 2021. Available from: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/symptoms/post-covid-19-condition.html
- Du H, Fang S, Wu S, Chen X, Chen J, Zhang Y, et al. Six-month follow-up of functional status in discharged patients with coronavirus disease 2019. BMC Infectious Disease. 2021;21:1271.
- McKnight PE, Kashdan TB. The importance of functional impairment to mental health outcomes: a case for reassessing our goals in depression treatment research. Clinical Psychology Review. 2009;29(3):243–59.
- Lam RW, Malhi GS, McIntyre RS, Demyttenaere K, Gorwood P, Michalak EE, et al. Fatigue and occupational functioning in major depressive disorder. Austrlian and New Zealand Journal of Psychiatry. 2013;47(11):989–91.
- Keltner D, Kring AM. Emotion, social function, and psychopathology. Review of General Psychology. 1998;2(3):320–42.
- Leppänen JM. Emotional information processing in mood disorders: a review of behavioral and neuroimaging findings. Current Opinion in Psychiatry. 2006;19(1):34–9.
- Pardo J V, Pardo PJ, Humes SW, I Posner M. Neurocognitive dysfunction in antidepressant-free, non-elderly patients with unipolar depression: alerting and covert orienting of visuospatial attention. Journal of Affective Disorder. 2006;92(1):71–8.
- Rose EJ, Ebmeier KP. Pattern of impaired working memory during major depression. Journal of Affective Disorders. 2006;90(2–3):149–61.
- Zimmerman M, McGlinchey JB, Young D, Chelminski I. Diagnosing major depressive disorder I: A psychometric evaluation of the DSM-IV symptom criteria. Journal of Nervous Mental Disease. 2006;194(3):158–63.
- Christensen L, Duncan K. Distinguishing depressed from nondepressed individuals using energy and psychosocial variables. Journal of Consulting and Clinical Psychology. 1995;63(3):495–8.
- Lerner D, Adler DA, Chang H, Lapitsky L, Hood MY, Perissinotto C, et al. Unemployment, job retention, and productivity loss among employees with depression. Psychiatric Services. 2004;55(12):1371–8.
- Menges D, Ballouz T, Anagnostopoulos A, Aschmann HE, Domenghino A, Fehr JS, et al. Burden of post-COVID-19 syndrome and implications for healthcare service planning: A population-based cohort study. PLoS One. 2021;16(7):e0254523.
- Clark DM. Realizing the Mass Public Benefit of Evidence-Based Psychological Therapies: The IAPT Program. Annual Review of Clinical Psychology. 2018;14:159–83.
- National Institute for Health and Care Excellence. Common mental health problems: identification and pathways to care [Internet]. 2011. Available from: http://www.nice.org.uk/guidance/cg123
- Hofmann SG, Asnaani A, Vonk IJJ, Sawyer AT, Fang A. The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses. Cognitive Therapy and Research. 2012;36(5):427–40.
- Li I, Millard M, Haskelberg H, Hobbs M, Luu J, Mahoney A. COVID-19 related differences in the uptake and effects of internet-based cognitive behavioural therapy for symptoms of obsessive-compulsive disorder. Behavioural and Cognitive Psychotherapy. 2022;50(2):219–36.
- Fenn K, Byrne M. The key principles of cognitive behavioural therapy. InnovAiT. 2013;6(9):579–85.
- Centre for Addiction and Mental Health. Cognitive behavioural therapy. [Internet]. [Cited 2022 April 27]. Available from: https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/cognitive-behavioural-therapy
- The Canadian Association of Cogntiive and Behavioural Therapies. National Guidelines for Training in CBT. [Internet] 2019 [Cited 2022 April 27]. Available from https://cacbt.ca/en/training/national-guidelines-for-training-in-cbt/
- Gratzer D, Khalid-Khan F. Internet-delivered cognitive behavioural therapy in the treatment of psychiatric illness. Canadian Medical Association Journal. 2016; 1;188(4):263 LP – 272.
- Beck JS. Cognitive Behavior Therapy: Basics and Beyond. Third. London, England: Guilford Press; 2020.
- Hofmann SG, Wu JQ, Boettcher H. Effect of cognitive-behavioral therapy for anxiety disorders on quality of life: a meta-analysis. Journal of Consulting and Clinical Psychology. 2014;82(3):375–91.
- DiMauro J, Domingues J, Fernandez G, Tolin DF. Long-term effectiveness of CBT for anxiety disorders in an adult outpatient clinic sample: a follow-up study. Behaviour Research and Therapy. 2013;51(2):82–6.
- Niles AN, Axelsson E, Andersson E, Hedman-Lagerlöf E, Carlbring P, Andersson G, et al. Internet-based cognitive behavior therapy for depression, social anxiety disorder, and panic disorder: Effectiveness and predictors of response in a teaching clinic. Behaviour Research and Therapy. 2021;136:103767.
- Zhang B, Ding X, Lu W, Zhao J, Lv Q, Yi Z, et al. Effect of group cognitive-behavioral therapy on the quality of life and social functioning of patients with mild depression. Shanghai Archives of psychiatry. 2016;28(1):18–27.
- Ezawa ID, Bartels GC, Strunk DR. Getting down to business: an examination of occupational outcomes in cognitive behavioral therapy for depression. Cognitive Behaviour Therapy. 2021;50(6):479–91.
- He J, Yang L, Pang J, Dai L, Zhu J, Deng Y, et al. Efficacy of simplified-cognitive behavioral therapy for insomnia(S-CBTI) among female COVID-19 patients with insomnia symptom in Wuhan mobile cabin hospital. Sleep and Breathing. 2021;25:2213–9.
- Liu Z, Qiao D, Xu Y, Zhao W, Yang Y, Wen D, et al. The Efficacy of Computerized Cognitive Behavioral Therapy for Depressive and Anxiety Symptoms in Patients With COVID-19: Randomized Controlled Trial. Journal of Medical Internet Research. 2021;23(5):e26883.
- Li J, Li X, Jiang J, Xu X, Wu J, Xu Y, et al. The Effect of Cognitive Behavioral Therapy on Depression, Anxiety, and Stress in Patients With COVID-19: A Randomized Controlled Trial. Frontiers in Psychiatry. 2020; 11(580827)
- Fan Y, Shi Y, Zhang J, Sun D, Wang X, Fu G, et al. The effects of narrative exposure therapy on COVID-19 patients with post-traumatic stress symptoms: A randomized controlled trial. Journal of Affective Disorders. 2021;293:141–7.
- Wu KK, Chan SK, Ma TM. Posttraumatic stress, anxiety, and depression in survivors of severe acute respiratory syndrome (SARS). Journal of Traumatic Stress. 2005;18(1):39–42.
- Hammond GC, Croudace TJ, Radhakrishnan M, Lafortune L, Watson A, McMillan-Shields F, et al. Comparative Effectiveness of Cognitive Therapies Delivered Face-to-Face or over the Telephone: An Observational Study Using Propensity Methods. PLoS One. 2012;7(9):e42916.
