
MINI REVIEW
By Denise DuBois & Zinnia Batliwalla
In 2016 the Ombudsman of Ontario released Nowhere to Turn (1), a report which lambasted the government about the residential crisis currently facing Ontario’s developmental sector. According to Nowhere to Turn, there are few system safeguards to ensure that adults with intellectual and developmental disabilities (IDD) are not inappropriately placed in long-term care (LTC) homes, nor are there proactive policies to support aging-in-place for adults with IDD (1). Recent statistics demonstrate that aging adults with IDD are placed in LTC at younger ages and at higher frequency than adults without IDD in Ontario (2).
A year after Nowhere to Turn’s release, the Ministry of Community and Social Services (MCSS) and the Ministry of Health and Long-Term Care (MOHLTC) jointly released Guidelines for Supporting Adults with a Developmental Disability When Applying To, Moving Into and Residing In a Long-Term Care Home.
Cross-sector collaborations, such as the development of these Guidelines, may support aging adults with IDD and their families to navigate the frequently siloed disability and aging sectors. The Guidelines provide an overview of both these sectors in Ontario and outline the process for applying to LTC. These Guidelines, however, do not address the existing gaps in residential service provision, nor account for the mounting demands of an aging population, currently challenging both sectors.
Adults with IDD are living longer and the population of adults with IDD over the age of 64 is expected to double in Ontario by 2021 (2). Due to the combined impacts of aging and IDD, these individuals often experience cognitive decline and frailty at a younger age (e.g., middle age) (3). As their needs increase, services from both the MOHLTC (e.g., home care, LTC) and the MCSS (e.g., group home, case management) may be required and overlap.
The majority of adults with IDD continue to live with their families well into adulthood (4). Currently, Ontario provides residential services for less than 30 per cent (18,000 persons) of the estimated total population of adults with IDD (1,5). Parents of individuals with IDD spend more time caregiving per week than any other informal caregivers in Canada (6). But, these caregivers are also aging (7) and are at significant risk of developing health problems due to their caregiving role (6). Aging caregivers may no longer be able to fulfill their role due to death, ill health, or the increasingly complex needs of their aging adult child (8). These changing needs may necessitate aging-in-place supports (e.g., home modifications, assistive technology, in-home care) (9) or relocation of the adult child to another residential setting (e.g., from group home or family home to LTC home) (10).

The developmental sector in Ontario is struggling to provide the quality and quantity of housing and associated supports required to serve an aging population (11). There are currently more than 14,000 adults waiting for provincially-funded residential placements (5). With few residential options available within the developmental sector, families of aging adults with IDD may see LTC as the most feasible option.
Aging adults with IDD may be unnecessarily prioritized for LTC. In Ontario, LTC homes are funded by the MOHLTC and provide adults with 24-hour nursing, personal care, and support with daily activities. Those 65 years of age and older are the primary residents of LTC homes (12), although in Ontario those admitted are most often over the age of 80 (2). From 2009 to 2013, adults with IDD were three to nine times more likely to be admitted to LTC in Ontario than those in the general population (2). The current assessment method used to prioritize those who require LTC relies on static measures of cognitive and functional abilities, which fails to account for the baseline needs of individuals with childhood-onset disabilities. Individuals with IDD are three times more likely to receive the highest prioritization level compared to those without IDD, despite being on average 20 years younger (2). Since LTC homes are set up to serve older, frailer individuals, as outlined in Nowhere to Turn, LTC homes may not have the staffing, programming, and supports required to address developmental needs (1).
Historically, the disability and aging fields have operated separately (13,14). There is recognition both in Nowhere to Turn and the empirical literature that bridging activities may support aging and disability sectors to address service gaps. Bridging strategies aim to share existing resources and to develop new knowledge in practice, policy, and research across disability (in this case, the developmental) and aging sectors (15). The field of aging is most often framed by a biomedical model of health, so interventions designed to benefit older adults have focused on preventing and curing medical problems causing disability (16,17). In contrast, the disability field has developed through a social model of health, which prioritizes inclusive environments and the reduction of systemic barriers.
Bridging activities attempt to cross-pollinate knowledge in both fields, which have been traditionally siloed in healthcare policy and administration, as well as research.
Bridging activities attempt to cross-pollinate knowledge in both fields, which have been traditionally siloed in healthcare policy and administration, as well as research. This may help both the aging with and aging into disability populations, as they have similar levels of functional difficulties (15) and thus, may benefit from the application or adaptation of a program or service used in the other field. Yet, little is known about the bridging strategies that have been described in the empirical literature regarding supporting aging adults with IDD prior to, during, or after residential transition.
Methods
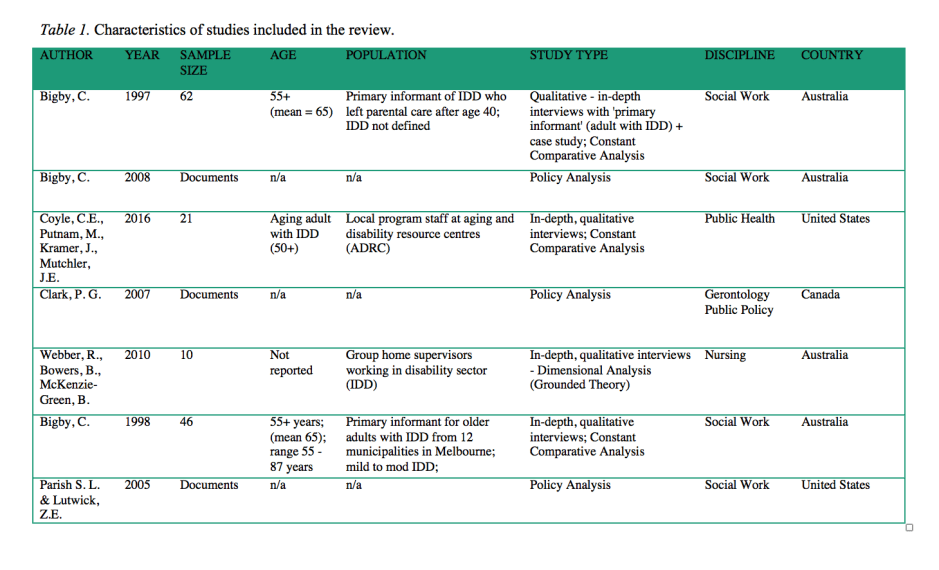
This review presents emerging themes from articles describing activities specifically related to supporting aging adults with IDD prior to, during, or after residential transition. The reviewed articles (N=7) were selected from a larger scoping review (18) dataset (N=48) (in progress) focused on characterizing bridging activities at the nexus of aging and disability. A systematic search of English, peer-reviewed publications using Medline, CINAHL, Embase, PsycInfo, Sociological Abstracts, and Cochrane Library yielded 9281 articles. All titles/abstracts were screened and 144 underwent full text review by two investigators. Forty-eight articles (1988 to 2017) met the inclusion criteria. Three investigators then reviewed all abstracts for terms: intellectual/developmental disabilities AND housing, home, LTC OR residential transition (and related terms based on MeSH headings) leading to the seven articles reviewed (1997 to 2016, see Table 1).
The following information was collected from each article: (a) bibliographic information including author, year of publication, geographical location, disciplinary background of first author, study design, and purpose; (b) population information including age group, sample size, and residence types; and (c) scope of information on bridging strategies including major disability and aging concepts, main findings (problems and strategies), conclusion of the study, and rehabilitation implications. A research technique known as qualitative content analysis was used to systematically extract and analyze the data. From this analysis, four themes emerged: (a) Unmet needs; (b) Bridging access to services/relationships; (c) Bridging knowledge; and (d) Bridging policies. These themes are summarized below.
 Findings
Findings
Theme 1 – Unmet Needs. Unmet needs exist for aging adults with IDD prior to and after transition to a LTC home. Broadly across the articles in this review, authors reported that adults with IDD were seen to have smaller informal networks and limited financial resources (7,19–23). As they aged, they often relied heavily on the supports of parents and service providers, partially because they are less likely to have a spouse or adult child who can provide informal caregiving supports.
Whether in a group home or family home setting, challenges to provide increased supports due to functional changes (e.g., chronic health needs; dementia; changes in work, recreational, and activities of daily living) have been reported to cause considerable strain for primary caregivers (7,19,23,24). This strain often led families to consider the few available residential alternatives.
Once an adult with IDD transitions to LTC, the environment may be seen to lack stimulation (e.g., recreation activities, socialization) since it is usually set up for much older, frailer individuals (19–22,25). Further, staff may not be trained or have enough time to support the communication and behavioural needs of adults with IDD. Concerns regarding ‘double dipping’ (19,20,22), where an individual receives overlapping benefits from two sectors, have also led to individuals losing developmental sector supports upon transition to LTC (22,26). Thus, adults with IDD living in LTC may find themselves with few people who can support them appropriately or advocate on their behalf (20).
Theme 2 – Bridging access to services and relationships. To meet the needs of this growing population, bridging strategies may improve access to services and relationships across sectors. Broadly, researchers have called for improved access to allied health, hospital, and specialist geriatric care services, particularly for those currently living in the community (7,19,21,23,25). For instance, Coyle and colleagues (7) suggested that generic aging programs (e.g., falls prevention, memory clinics) should be expanded so that more adults with IDD can access them. For improved access to effective care, more professionals (e.g., rehabilitation, medical) would require training on best practices for serving this population, and governments would need to invest in integrated models of care (7,22). Bigby (22) suggested that jurisdictions consider the adoption of the United Kingdom’s approach where all adults with IDD are served across the lifespan by community-based specialist interdisciplinary teams.
Promoting relationships between service providers across the aging and disability sectors was also described. Authors suggested (a) considering the entire family unit, rather than only the individual with IDD (7,22), (b) allowing service providers in the developmental sector to continue providing social and emotional supports after transition to LTC (19–21), and (c) developing liaison positions to facilitate appropriate inpatient care and adaptation of specialist geriatric services (22).
Theme 3 – Bridging knowledge. Bridging knowledge through cross collaborations may increase the number of service providers with experience serving adults with IDD, and enhance their knowledge to support aging adults with IDD (7,20–24,26). At a practical level, knowledge of assessing and modifying the environment to promote aging-in-place, or to ensure an appropriate person-environment fit within a LTC home, is necessary for the ‘younger old’ who remain mobile and active (7,19,20,22). Without an option to age-in-place, individuals with IDD may be forced to enter LTC, which often prioritizes medical care rather than an environment that promotes community integration and recreation.
Other bridging strategies that were suggested to improve knowledge sharing included (a) developing close working relationships at multiple levels of the system from frontline staff to policy makers (7,19,21,22), (b) researching current service gaps to demonstrate where integration can be improved (7), and (c) promoting principles of aging-in-place within the developmental sector through the use of environmental adaptation, home modifications, and equipment (19,22).
Theme 4 – Bridging policies. To ensure bridging strategies are implemented, formal policies are often required. Some jurisdictions such as Victoria, Australia, have formal policies for aging-in-place (22) specific to adults with IDD, while Ontario does not (24). Two studies suggest that proactive aging-in-place policies should be supported at both national and regional levels (22,24). These policies should include earmarking of funds within the developmental sector. These funds would compensate for the additional age-related needs of adults with IDD and to promote aging-in-place (22,24). Such transfers may ensure that the ‘younger old’ can live in family or group home settings for longer and that inappropriate placements in LTC are delayed or prevented. Finally, and specific to Canada’s system, increased cooperation and coordination over the common values of home care policy may bridge the disability and aging sectors, which have largely run on “parallel and non-intersecting paths, but are now converging as a result of aging societies” (24).
Practice Implications
How does this relate to what’s happening in Ontario? The new inter-ministerial Guidelines represent a first attempt to bridge policies across sectors and highlights a move towards more formalized partnerships between ministries. While these Guidelines may clarify how the system currently works, they do not outline specific activities to bridge disability and aging fields in practice. This review summarized a range of bridging strategies related to service access, policies, and knowledge (e.g., skills, philosophies of care), which may be applied within the Ontario system to prepare for and serve the current unmet health, housing, and rehabilitation needs of adults with IDD.
What is the role for rehabilitation? As demonstrated by several strategies in this review, the rehabilitation field – which aims to optimize function – transcends the boundaries of the siloed aging and disability fields (27). For this reason, rehabilitation professionals are uniquely positioned to facilitate knowledge sharing as ‘boundary spanners’. They may inform bridging strategies through (a) models of service delivery, (b) policies related to aging, disability, and housing, and (c) prevention and maintenance of function based on person-centred principles of care.
Bridging the fields of aging and disability is essential to ensure that residential settings are attuned to the needs of aging adults with IDD. In Ontario, aging adults with IDD and their families encounter a patchwork of programs and services which may result in inappropriate LTC placement. Efforts to bridge the fields of aging and disability may delay or prevent adults with IDD from entering LTC inappropriately by promoting policies of aging-in-place, or by prioritizing person-environment fit within the LTC settings.
References
- Dube P. Nowhere to turn. Investigation into the Ministry of Community and Social Services’ response to situations of crisis involving adults with developmental disabilities. Ombudsman Ontario Report. 2016.
- Ouellette-Kuntz H, Martin L, McKenzie K. Aging Project Final Report. Toronto, ON: Health Care Access Research and Developmental Disabilities Program; 2016.
- McKenzie K, Ouellette-Kuntz H, Martin L. Using an accumulation of deficits approach to measure frailty in a population of home care users with intellectual and developmental disabilities: An analytical descriptive study. BMC Geriatr. 2015;15:170.
- Lakin KC, Stancliffe RJ. Residential supports for persons with intellectual and developmental disabilities. Mental Retardation and Developmental Disabilities Research Reviews. 2007.
- Auditor General of Ontario. Residential services for people with developmental disabilities. 2013;332-61.
- MaRS Solutions Lab. Residential support for adults with developmental disability. 2014;(April):1-21.
- Coyle CE, Putman M, Kramer J, Mutchler JE. The role of aging and disability resource centers in serving adults aging with intellectual disabilities and their families: Findings from seven states. J Aging Soc Policy. 2016;28(1):1-14.
- Woodman AC, Mailick MR, Anderson KA, Esbensen AJ. Residential transitions among adults with intellectual disability across 20 years. Am J Intellect Dev Disabil. 2014;119(6):496-515.
- Hammel J, Lai J-S, Heller T. The impact of assistive technology and environmental interventions on function and living situation status with people who are aging with developmental disabilities. Disabil Rehabil. 2002;24(1/2/3):93–105.
- Heller T, Sorensen A. Promoting healthy aging in adults with developmental disabilities. Dev Disabil Res Rev. 2013;18(1):22–30.
- Patti PJ, Amble KB, Flory MJ. Life events in older adults with intellectual disabilities: Differences between adults with and without Down Syndrome. J Policy Pract Intellect Disabil. 2005;2(2):149–55.
- Legislative Assembly of Ontario. Select Committee on Developmental Services Final Report. Toronto, ON; 2014.
- Bickenbach J, Bigby C, Salvador-Carulla L, Heller T, Leonardi M, Leroy B, et al. The Toronto declaration on bridging knowledge, policy and practice in aging and disability. Int J Integr Care. 2012;12:e205.
- Zola IK. Aging and disability: Toward a unifying agenda. Educ Gerontol. 1988;14(5):365–87.
- Putnam M. Bridging network divides: Building capacity to support aging with disability populations through research. Disabil Health J. 2014;7(S1):1–15.
- Naue U, Kroll T. Bridging policies and practice: Challenges and opportunities for the governance of disability and ageing. Int J Integr Care. 2010;10:e041.
- Monahan DJ, Wolf DA. The continuum of disability over the lifespan: The convergence of aging with disability and aging into disability. Disabil Health J. 2014;7(S1):S1–3.
- Nalder EJ, Putnam M, Salvador-Carulla L, Spindel A, Batliwalla Z, Lenton E. Bridging knowledge, policies and practices across the ageing and disability fields: A protocol for a scoping review to inform the development of a taxonomy. BMJ Open. 2017;7(10):e016741.
- Webber R, Bowers B, McKenzie-Green B. Staff responses to age-related health changes in people with intellectual disability in group homes. Disabil Soc. 2010;25(6):657–71.
- Bigby C. Later life for adults with intellectual disability: A time of opportunity and vulnerability. J Intellect Dev Disabil. 1997;22(2):97–108.
- Bigby C. Shifting responsibilities: The patterns of formal service use by older people with intellectual disability in Victoria. J Intellect Dev Disabil. 1998;23(3):229–43.
- Bigby C. Beset by obstacles: A review of Australian policy development to support ageing in place for people with intellectual disability. J Intellect Dev Disabil. 2008;33(1):76–86.
- Parish SL, Lutwick ZE. The emerging crisis in long-term care for people with developmental disabilities: A critical analysis of the emerging crisis in long-term care for people with developmental disabilities. Soc Work. 2005;50(4):345–54.
- Clark PG. Understanding aging and disability perspectives on home care: Uncovering facts and values in public-policy narratives and discourse. Can J Aging. 2007;26(S1):47–62.
- Bigby C, Wilson NJ, Balandin S, Stancliffe RJ. Disconnected expectations: Staff, family, and supported employee perspectives about retirement. J Intellect Dev Disabil. 2011;36(3):167–74.
- Webber R, Bowers B, McKenzie-Green B, Cdso F. Staff responses to age-related health changes in people with an intellectual disability in group homes. Disabil Soc. 2010;25(6):657–27. Stucki G, Bickenbach J, Gutenbrunner C, Melvin J. Rehabilitation: The health strategy of the 21st century. J Rehabil Med. 2017.
