Knowledge Summary
By Lisbeth Alexandra Pino Gavidia
According to the Joint United Nations Programme on HIV/AIDS – UNAIDS, 1.7 million people around the globe were HIV positive in 2019 (1). In the same year, there was a 21% increase in new HIV infections in Latin America since 2010 (1). Latin America is a multicultural region populated by approximately 42 million Indigenous peoples, representing nearly 7.8% of the total population (2). While the HIV prevalence tended to be low (<1%), such as in Brazil 0.13%, pockets of high prevalence (>5%) were observed in some Indigenous communities (3). For example, 9.6% in Warao Venezuela, 7.5% in Chayahuita Peru, and 7.0% in Wayuu Colombia (4,5,6).
Gender, ethnicity, education, employment, housing, and health services are social determinants of health that interact to impact the health and well-being of Indigenous peoples in Latin America. For example, women’s important contributions to their Indigenous communities include farm labour, childcare, and family meal preparation. Despite these contributions, women in Indigenous communities often suffer a lack of education and occupation due to poverty (2). Additionally, the arduous daily labour routine is a barrier to accessing healthcare. The life roles and challenges of Indigenous women are closely linked to their unpaid family responsibilities, leaving little opportunity to access education and healthcare (2). These can be crucial social determinants of health that increase the vulnerability of Indigenous communities in general to HIV/AIDS.
Rocio’s case vignette will be used to present the complex problem of HIV within Indigenous communities. Spanish names are fictional and support the Latin American rural context: Suyay means hope, and Quechua is the Indigenous language spoken in Colombia, Ecuador, Peru, Bolivia, Chile, and Argentina. I will be using my framework called The Tree of Life to identify the protective factors shaping health and well-being. The Tree of Life framework is a creative solution to facilitate context-specific strategies within the model’s multi-level system as there is a need to better understand how context affects health outcomes. This vignette is the result of my missionary work to reach those who are marginalized in the Indigenous communities of Ecuador.
Case Vignette: Rocio
Rocio is a 23-year-old Indigenous woman who was diagnosed as HIV positive. Born and raised in the small, rural community of Suyay with a low socioeconomic status, Rocio spent much of her time taking care of her young siblings. With respect to gender roles, expectations put on her included living a life of household chores such as cleaning, drying, winnowing (remove the chaff from the wheat), threshing (grain gathering), and storing the family crops. Rocio’s early engagement in unpaid labour limited her ability to study in the closest high school.
Rocio married at the age of 20, and the cycle of poverty was repeated in her marriage. Any opportunity to form a connection with her husband and build a lasting relationship was always interrupted by his urgency to find a job in the urban areas. One day, he just never returned. Rocio felt hopeless in a house that lacked the basic services of an indoor toilet and clean water.
Rocio suddenly began experiencing weight loss, extreme exhaustion, recurring fever, and frequent diarrhea. Initially, she considered that perhaps her poor nutrition or workload on the farm was causing these symptoms, but they persisted and worsened over time. The physical effort to travel the half-hour by canoe from the Suyay community to the Quechu Health Centre (QHC) was a contributing factor to her declining emotional well-being.
Rocio managed to reach the QHC even while experiencing extreme exhaustion and anxiety. The doctor at the QHC, who had been practicing medicine for several years, performed a rapid blood test which determined that Rocio was infected with HIV. As the understanding of her HIV status dawned on her, she felt her life falling apart with the new knowledge that her time alive may be significantly shortened, especially without treatment.
Ester, the community health worker (CHW), reassured Rocio that she could be treated with antiretroviral therapy (ART) to slow the HIV virus from advancing to immunodeficiency syndrome (AIDS). Rocio was still afraid as she had never heard of this treatment. Ester was understanding of Rocio’s hesitancy and took the time to explain how antiretroviral medicine works. Indeed, her kindness helped Rocio build confidence that it is possible to live a happy, productive, and rewarding life. Ester’s compassionate approach helped break the barrier of stigma and discrimination for people like Rocio living with HIV/AIDS (7).
Rocio refused to become discouraged and was inspired to take a leadership role in her new circumstances. Her sense of belonging to the Suyay community empowered her to raise awareness of HIV/AIDS and increase traditional perspectives about sexuality. Rocio especially emphasized the spiritual component to health and well-being, knowing the serious health risks which can result when people isolate themselves from the spirit. “To focus on the spirit is like a tree firmly planted by streams of water, which leaves do not wither, neither fail to bear fruit,” she explained.
Rocio made significant improvements in her community, such as helping facilitate transfers to the QHC. Transfers included patients already diagnosed with HIV seeking additional care, patients who wanted to be tested for HIV, and newly diagnosed HIV patients. Rocio’s close interaction with the community allowed her to win trust, and her actions built community engagement to increase care-seeking behaviour within the Susay community. In the same way that Rocio was determined to live in the spirit by serving others, she hopes to inspire generations to come. Now, she has decided to pursue health education.
“To focus on the spirit is like a tree firmly planted by streams of water, which leaves do not wither, neither fail to bear fruit”
The Tree of Life in Shaping Health and Well-Being
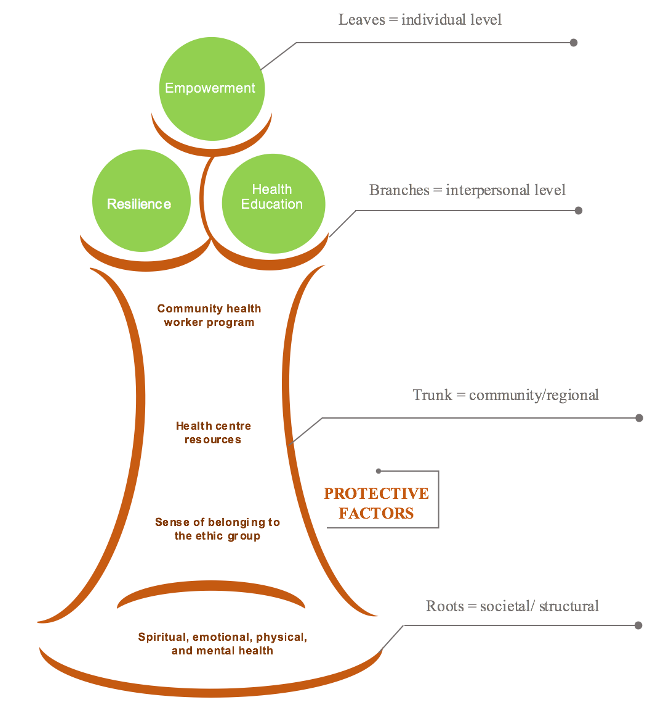
To consider the context in which Indigenous peoples strive to achieve health is important for creating strategies in rural communities. The protective factors among Indigenous populations from Latin American can be better understood using my tree framework based on a social-ecological model (8). Within this framework, health is built at multiple levels of society, represented by multiple zones of the tree: the roots, the trunk, the branches, and the leaves (Figure 1). Protective factors which have a foundation in the spiritual component may best serve to facilitate positive health outcomes.
The societal level is represented by the roots of the tree. To have a healthy tree, the roots should be healthy, including the values of Indigenous peoples that establish four components for human wholeness: spiritual, emotional, physical, and mental. When these four components are not in harmony, Indigenous peoples are in jeopardy of having poor health. The roots of the tree directly influence the trunk, just as the society within a country directly affects the health of the community. The trunk represents the community that is facilitating conditions to provide a sense of belonging to the ethnic group, health centre resources, and community health worker programs. The interpersonal or family level is represented by the branches of the tree. These include building relationships from the inside (community) to the outside (health centre).
The individual level is represented by the leaves of the tree. These are the fruits of the spirit that contribute to the leaves being healthy: peace, joy, patience, love, kindness, faithfulness, and self-control. Just as a tree cannot be healthy if all its leaves are dead, society cannot be healthy if all its individuals are sick. The vulnerable situations of Indigenous women resulted in health disparities and poorer health outcomes (9). This tree framework illustrates how HIV/AIDS requires the combination of protective factors within a multi-level system, as depicted by The Tree of Life in Figure 1.
The challenge, in this case, is the delivery of community-based approaches that support the rehabilitation process from the community to influence the social context (10). Health programs and interventions should aim to consider the context in which individuals and families strive to improve their health (11). The protective factors to keep in step with the spirit embedded in Rocio’s story can help inform prevention strategies to get comprehensive and compassionate care for people with HIV/AIDS.
Health is not only determined by individual factors but also by family, community, and society level factors. The narrative of Rocio, an Indigenous woman who was diagnosed with HIV/AIDS, helps us understand that rural agricultural livelihoods and isolation were barriers to accessing education and getting healthcare, which increases the risk factors of HIV. The protective factors are the primary contributors to health. A key component of health and well-being is to take into account the spiritual, which is fundamental for the quality of life in Indigenous communities. Health interventions in Indigenous communities should consider the social determinants of health and the importance of involving women in leadership roles to create the conditions for compassionate care and community involvement.

Acknowledgements
Featured illustration by Daniela Casas for rehabINK.
To refer to this article, it can be cited as:
Pino Gavidia, LA. rehabINK. HIV/AIDS from the Perspective of Indigenous Peoples in Latin America: A Compassionate Approach to Addressing Health and Well-Being. 2021:11. Available from: https://rehabinkmag.com
References
1. UNAIDS Data 2020 [Internet]. Geneva, Switzerland: UNAIDS Joint United Nations Programme on HIV/AIDS; 2020 Jul [cited 2021 April 19]. Available from: https://www.unaids.org/en/resources/documents/2020/unaids-data
2. Freire GN, Schwartz SD, Zumaeta M, Costa DC, Lundvall JM, Viveros MC, et al. Indigenous Latin America in the twenty-first century: the first decade [Internet]. Washington, DC. United States: The World Bank; 2016 Feb [cited 2021 April 19]. Available from: https://documents.worldbank.org/en/publication/documents-reports/documentdetail/145891467991974540/indigenouslatin-america-in-the-twenty-first-century-the-first-decade
3. Benzaken AS, Sabidó M, Brito I, Bermúdez XP, Benzaken NS, Galbán E, Peeling RW, Mabey D. HIV and syphilis in the context of community vulnerability among indigenous people in the Brazilian Amazon. International Journal for Equity in Health. 2017;16(1):1–9.
4. Villalba JA, Bello G, Maes M, Sulbaran YF, Garzaro D, Loureiro CL, Rangel HR, De Waard JH, Pujol FH. HIV-1 epidemic in Warao Amerindians from Venezuela: spatial phylodynamics and epidemiological patterns. AIDS. 2013;27(11):1783–91.
5. Zavaleta C, Fernández C, Konda K, Valderrama Y, Vermund SH, Gotuzzo E. High prevalence of HIV and syphilis in a remote native community of the Peruvian Amazon. The American Journal of Tropical Medicine and Hygiene. 2007;76(4):703–5.
6. Lobo García K, Pinzón J, Ramirez Bedoya B, Garrido VM, Manjarrés Barros VA, Haag Lederer AF. An educational strategy to raise awareness about sexual and reproductive health, HIV/AIDS, aimed at women in a Wayuu indigenous community in Colombia. XVII
International AIDS Conference, Mexico City, Mexico, August 3–8, 2008. Abstract No. CDC0922.
7. Kok MC, Dieleman M, Taegtmeyer M, Broerse JE, Kane SS, Ormel H, Tijm MM, De Koning KA. Which intervention design factors influence performance of community health workers in low-and middle-income countries? A systematic review. Health Policy and Planning. 2015;30(9):1207–27.
8. Bronfenbrenner U. The ecology of human development: experiments by nature and design. Cambridge, MA: Harvard University Press; 1979.
9. Weismantel MJ. Food, gender, and poverty in the Ecuadorian Andes. Philadelphia: University of Pennsylvania Press; 1989.
10. Mayaud P, Mabey D. Approaches to the control of sexually transmitted infections in developing countries: old problems and modern challenges. Sexually Transmitted Infections. 2004;80(3):174–82.
11. Pokhrel P, Regmi S, Piedade E. HIV/AIDS prevention in the Nepalese context. Evaluation & The Health Professions. 2008;31(2):198–210.
