
Commentary
By Stephanie Saunders, Cassandra D’Amore & Ava Mehdipour
Background
The Canadian Society for Exercise Physiology (CSEP) introduced new 24-hour movement guidelines in October 2020 to encourage Canadians to move as much as possible, in any way possible (1)! These guidelines are unique in that they offer direction for balancing movement-related behaviours, including physical activity (PA), sedentary behaviour, and sleep, in a complete 24 hours. The guidelines for older adults (65 years) highlight the benefits of regular PA to help mitigate physical and cognitive decline that occurs naturally as we age, such as reduced mobility and increased risk for chronic disease, and depression (2). However, it may be daunting for some older adults to be regularly physically active. As a result, the new guidelines advocate for light PA, which offers a lower intensity in contrast to moderate or vigorous PA (e.g., higher intensity), as a way for older adults to gain benefits from PA. In this commentary we emphasize the importance of light PA in the Canadian 24-hour movement guidelines for older adults, highlight the benefits of light PA, and discuss how light PA may be incorporated into rehabilitation settings.
Canadian 24-Hour Movement Guidelines
Canada’s new 24-hour movement guidelines were released to encourage Canadians to “make their whole day matter” (2). With respect to PA, the previous recommendations remain; 150 minutes of moderate to vigorous PA per week, muscle strengthening activities at least twice a week, and physical activities that challenge balance. There is also a new endorsement for obtaining several hours of light PA per day, including standing activities. In addition to the PA suggestions, the guidelines recommend limiting sedentary time to 8 hours or less, with less than 3 hours of recreational screen time, and getting 7 to 8 hours of sleep while maintaining a consistent sleep-pattern. Although there is an emphasis on increasing PA, these guidelines are among the first to recognize that we have a finite amount of time in each day where we balance a variety of movement-related behaviours. Instead of focusing on only changing one movement-related behaviour, the guidelines encourage Canadians to consider striving to reach each of the recommendations by substituting certain movement-related behaviours for others (e.g., sitting for standing). These trade-offs are important since each of the movement-related behaviours have their own distinct influence on health and so it is important to consider how changes in one can influence another (e.g., increasing walking time decreases sedentary time) (2). While PA is beneficial for most individuals, these guidelines may not apply to everyone. If you are unsure whether they apply to you, reach out to your healthcare provider.
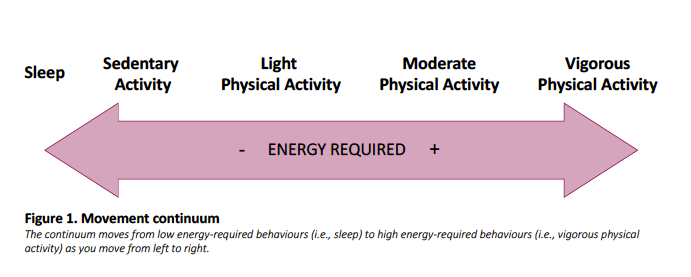
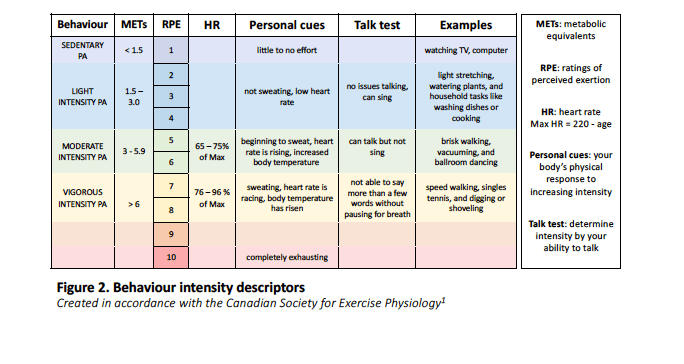
The movement-related behaviours discussed in the guidelines exist along a continuum shown in Figure 1. On the left, behaviours like sleeping require the least amount of energy or effort to complete and are considered less intense. Moving along the continuum to the right, these behaviours require more energy or become more intense. Physical activities fall across a broad section of this continuum representing the different intensity levels described in the guidelines. PA intensity can be defined using both relative and absolute scales. Relative scales can include a rating of perceived exertion (RPE), where an individual rates how hard they believe they are working on a scale of no effort to highest possible effort. There are multiple ways to identify relative intensity levels including the talk test and using personal cues (see Figure 2 for more details). Conversely, absolute scales include metabolic equivalents (METs), which is the ratio of energy expenditure compared to rest. Or using per cent of heart rate max (see Figure 2 for more details). Figure 2 describes each intensity level across these measures. While absolute scales are key for clinical research, relative scales are helpful for individuals trying to assess their own level of effort. Understanding how to translate between these relative and absolute measures may be helpful for promoting different PA intensities.
Benefits of Light PA
While PA of any kind is beneficial, recent research has emerged highlighting the benefits of light PA. Researchers have shown that light PA is beneficial regardless of how physically active one is overall. Light PA not only improves overall well-being (3,4), but higher amounts of total time spent in light PA can help reduce the risk of early mortality (4,5). Further, multiple studies have demonstrated that light PA can improve dynamic balance (e.g., walking over uneven surfaces) and static balance (e.g., holding an awkward object) (6,7), while protecting against cognitive decline and depression (6,8).
The literature also suggests that replacing sedentary time with light PA (e.g., talking on the phone while walking rather than sitting) demonstrates the greatest health benefits (3). This is because both long stretches of time (e.g., sitting at a desk for 8 hours straight) and total accumulated time (e.g., low levels of overall PA) spent being sedentary can be harmful to one’s health, leading to an increased risk of cardiovascular disease, obesity, dysmobility syndrome, and mortality (9). By substituting movement-related behaviours we can reduce the negative impacts of being highly sedentary.
Another distinct advantage of light PA is that most older adults can partake in it, regardless of their capacity. Older adults may experience reduced capacity as they are more likely to be managing multiple health conditions at once (10), or they may have been physically inactive. Regardless of whether older adults have reduced capacity or not, engaging in light PA may be less intimidating than higher intensity activities. This is because benefits are accrued through simply breaking up long stretches of sedentary time. In many cases the goal is to accumulate minutes per day that add up to hours, rather than single long bouts of PA. Simple ways older adults can replace sedentary time with light PA include hourly standing breaks, marching on the spot during stationary activities, or standing instead of sitting during chores, screen, or recreation activities (see Figure 2 for more examples).

Light PA in Healthcare and Rehabilitation
Healthcare providers play a key role in supporting older adults’ engagement in PA. Healthcare providers can teach older adults how to recognize the different types of PA using RPE’s and then offer recommendations on how to incorporate PA at the appropriate intensity. A common place to start is by suggesting light walking a few times per week within an RPE of 2-5, as older adults have regularly reported walking as the most preferred method of engaging in PA (11).
In addition, light PA often aligns with preferred occupational activities (e.g., chores or hobbies) and thus Occupational Therapists may be essential for helping older adults to incrementally replace sedentary behaviours with meaningful light PA. For instance, helping older adults regain function for gardening activities.
Physiotherapists (PTs) may be critical for encouraging older adults to begin light PA programs and then incrementally increase both the volume and intensity. For example, PTs may start a walking program by recommending usual pace walking at first, then, once deemed appropriate, they may suggest increasing intensity as dictated by RPEs and incorporating more challenging terrain.
Primary care providers (PCPs), such as family doctors or nurse practitioners, may also support older adults by encouraging habitual light PA during regular check-ups and through exercise prescriptions, which have shown to increase uptake of PA (for resources on exercise prescriptions see: www.exerciseismedicine.org) (12). Further, PCPs can direct older adults to rehabilitation experts and offer insight on how to safely engage in PA for those with chronic conditions or reduced capacity. Indeed, there is a substantial body of literature supporting the benefits of PA for individuals with a variety of health conditions (e.g., cancer, stroke, spinal cord injury, cardiac disease, diabetes, frailty) (13-17). To this end, healthcare providers can be assured that recommending PA is safe and light PA is manageable for most individuals.
The growth of virtual PA programs during the ongoing COVID-19 pandemic (18) has created opportunities to engage in regular PA, even with the closure of recreation facilities. Light PA may be a central component of these virtual programs, as it is less strenuous and typically requires less equipment, reducing the need for a healthcare provider or exercise instructor to be physically present with the individual. Healthcare providers are also using virtual systems to connect with older adults who cannot access in-person resources due to government restrictions (e.g., physical distancing guidelines), living environment (e.g., living in a remote area), or personal reasons (e.g., fear of contracting COVID-19) (19). These systems seem to be amenable to older adults, offering them a chance to engage in supervised therapy (20). In terms of those seeking online leisure activities, virtual PA programs offered through community partners and gyms can provide opportunities for older adults to engage in PA and gain social support throughout the process (see end of article for local links) (21).
Conclusions
Many people know they should be physically active, but there is a gap between knowing and doing. Getting started is often the hardest part, especially for those who have taken a break or are new to PA. Breaking down the different intensities of PA and advocating for small steps, like replacing sedentary behaviour with light PA, is a crucial component to encourage Canadians to incrementally increase the total amount of PA they engage in. Importantly, researchers and healthcare providers, including rehabilitation therapists, are uniquely positioned to promote this message and implement these incremental changes in their practice.
Resources
If you or an older adult you know is looking to become more physically active please see these additional resources:
- Virtual Y programs ywearehere.ca
- Community exercise programs out of the University of Toronto: https://www.physicaltherapy.utoronto.ca/research/ktalab/ongoing-research/community-exercise-programs/
- Online Physical activity programs out of McMaster University (https://pace.mcmaster.ca/mcmaster-pace-live-at-home/)
- McMaster optimal aging portal (https://www.mcmasteroptimalaging.ca/ )
- 24-Hour Movement Guidelines for older adults: https://csepguidelines.ca/adults-65/
- 24-Hour Movement Guidelines: https://www.youtube.com/watch?v=uZwioD6_f28
Acknowledgements
Featured illustration by Daniela Casas for rehabINK.
To refer to this article, it can be cited as:
Saunders S, D’Amore C, Mehdipour A. 24-Hour Canadian Movement Guidelines and the Benefits of Light Physical Activity for Older Adults. rehabINK. 2021:11. Available from: https://rehabinkmag.com
References
- Canadian Society for Exercise Physiology. Canadian 24-Hour Movement Guidelines: Glossary of Terms 2021 [Internet]. Available from: https://www.csep.ca/en/guidelines/glossary-2017.
- Ross R, Chaput J-P, Giangregorio LM, Janssen I, Saunders TJ, Kho ME, et al. Canadian 24-Hour Movement Guidelines for Adults aged 18–64 years and Adults aged 65 years or older: an integration of physical activity, sedentary behaviour, and sleep. Applied Physiology, Nutrition, and Metabolism. 2020;45(10):S57-S102.
- Buman MP, Hekler EB, Haskell WL, Pruitt L, Conway TL, Cain KL, et al. Objective Light-Intensity Physical Activity Associations With Rated Health in Older Adults. American Journal of Epidemiology. 2010;172(10):1155-65.
- Ku P, Hamer M, Liao Y, Hsueh M, Chen L. Device-measured light-intensity physical activity and mortality: A meta-analysis. Scand J Med Sci Sports. Scandinavian Journal of Medicine Science in Sports. 2020;30(1):13-24.
- Ekelund U, Tarp J, Steene-Johannessen J, Hansen BH, Jefferis B, Fagerland MW, et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. British Medical Journal. 2019;366.
- Gando Y, Yamamoto K, Murakami H, Ohmori Y, Kawakami R, Sanada K, et al. Longer time spent in light physical activity is associated with reduced arterial stiffness in older adults. Hypertension. 2010;56(3):540-6.
- Pau M, Leban B, Collu G, Migliaccio GM. Effect of light and vigorous physical activity on balance and gait of older adults. Archives of Gerontology and Geriatrics. 2014;59(3):568-73.
- Stubbs B, Chen L-J, Chang C-Y, Sun W-J, Ku P-W. Accelerometer-assessed light physical activity is protective of future cognitive ability: A longitudinal study among community dwelling older adults. Experimental Gerontology. 2017;91:104-9.
- de Rezende LFM, Rey-López JP, Matsudo VKR, do Carmo Luiz O. Sedentary behavior and health outcomes among older adults: a systematic review. BioMed Central Public Health. 2014;14(1):1-9.
- Nicholson K, Griffith LE, Sohel N, Raina P. Examining early and late onset of multimorbidity in the Canadian Longitudinal Study on Aging. Journal of the American Geriatrics Society. 2021.
- Amireault S, Baier JM, Spencer JR. Physical activity preferences among older adults: A systematic review. Journal of Aging and Physical Activity. 2018;27(1):128-39.
- Lee PG, Jackson EA, Richardson CR. Exercise prescriptions in older adults. American family physician. 2017;95(7):425-32.
- Patel AV, Friedenreich CM, Moore SC, Hayes SC, Silver JK, Campbell KL, et al. American College of Sports Medicine roundtable report on physical activity, sedentary behavior, and cancer prevention and control. Medicine and science in sports and exercise. 2019;51(11):2391.
- Gordon NF, Gulanick M, Costa F, Fletcher G, Franklin BA, Roth EJ, et al. Physical activity and exercise recommendations for stroke survivors: an American Heart Association scientific statement from the Council on Clinical Cardiology, Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention; the Council on Cardiovascular Nursing; the Council on Nutrition, Physical Activity, and Metabolism; and the Stroke Council. Circulation. 2004;109(16):2031-41.
- Ginis KM, Hicks A, Latimer A, Warburton D, Bourne C, Ditor D, et al. The development of evidence-informed physical activity guidelines for adults with spinal cord injury. Spinal Cord. 2011;49(11):1088-96.
- LeRoith D, Biessels GJ, Braithwaite SS, Casanueva FF, Draznin B, Halter JB, et al. Treatment of diabetes in older adults: an endocrine society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism. 2019;104(5):1520-74.
- Dent E, Morley J, Cruz-Jentoft A, Woodhouse L, Rodríguez-Mañas L, Fried L, et al. Physical frailty: ICFSR international clinical practice guidelines for identification and management. The Journal of Nutrition, Health & Aging. 2019;23(9):771-87.
- Prvu Bettger J, Resnik LJ. Telerehabilitation in the age of COVID-19: an opportunity for learning health system research. Physical Therapy. 2020;100(11):1913-6.
- Webster P. Virtual health care in the era of COVID-19. The Lancet. 2020;395(10231):1180-1.
- Moffet H, Tousignant M, Nadeau S, Mérette C, Boissy P, Corriveau H, et al. Patient satisfaction with in-home telerehabilitation after total knee arthroplasty: results from a randomized controlled trial. Telemedicine and e-Health. 2017;23(2):80-7.
- Sepúlveda-Loyola W R-SI, Pérez-Rodríguez P, Ganz F, Torralba R, Oliveira D V., et al. . Impact of Social Isolation Due to COVID-19 on Health in Older People: Mental and Physical Effects and Recommendations. Journal of Nutrition Healing and Aging. 2020.
