
ORIGINAL RESEARCH
By Brydne Morgan Edwards, Qianwei (Stella) Wang & Deborah Hébert
Many stroke survivors experience ongoing functional limitations due to spasticity. Spasticity is a movement disorder associated with brain injuries, whereby muscles contract involuntarily (1,2). It impacts the ability to use the hands and arms for daily tasks like cooking and bathing. These functional challenges can reduce quality of life (1).
Occupational therapists (OTs) use upper extremity orthoses (UEOs) – such as static splinting – to help manage pain and to minimize the negative, and often irreversible, impacts of prolonged spasticity, such as contractures. Contractures occur when there is permanent shortening of muscle fibres. This shortening limits range of motion and make daily self-care tasks such as washing and nail trimming difficult (2,3).
“I would say I’m doing overall much less static splinting … than I did ten years ago … I’m just not sure that the literature is supporting it … that being said though, there’s still some cases [where it works].”
– Lucy, OT
Despite the frequent use of UEOs, recent literature suggests that they may not have a therapeutic impact on spasticity. A splint, a common type of UEO, is a device applied to modify or maintain the position of the hand or arm. UEOs control abnormal movements of one or more body segments around a joint to maintain specific limb positions (4). Early research documenting the effectiveness of UEOs suggested that they were effective at: (a) inhibiting abnormal movements caused by spasticity; (b) preventing contractures; (c) reducing pain; and (d) improving daily function (5). Yet, more recent evidence suggests that UEOs may not be as effective in managing spasticity after stroke as once thought (3-5). A therapists’ clinical assessment for and choice of an UEO likely contribute to the overall impact of an UEO on spasticity. To date, however, these clinical decision-making factors have been largely unexplored (6-8).
This article aimed to understand whether and why OTs use UEOs to manage post-stroke spasticity. Using a descriptive qualitative approach, it explores (a) OTs’ experiences and perspectives about clinical goals they hope to achieve with UEOs, (b) how they make decisions about UEO design, and (c) to identify client and environmental factors that influence intervention planning.
Following Research Ethics Board approval from the University of Toronto, 10 Canadian OTs working with adults with spasticity from stroke or other acquired brain injuries were recruited and consented to be interviewed. All but one participant had at least 10 years of experience. These participants worked in different clinical settings, including community, outpatient rehabilitation, and inpatient rehabilitation. Participants engaged in one semi-structured phone interview between January and April 2013. Analysis of the transcribed interviews, uncovered three themes related to OTs’ decision-making around UEOs (11).
Different assumptions lead to different guiding principles
The wearing schedule and UEO design were influenced by participants’ assumptions about how UEOs could be used to manage spasticity. The OTs (who have been given pseudonyms) described three underlying assumptions about how UEOs manage spasticity, which had implications for UEO design and recommendations for use. Four of the OTs reported that UEOs should only be used overnight to prevent unnecessary immobilization that could contribute to contractures. They believed that stretching exercises and movement during daily activities would enhance functional use of the arm and hand. For example, “… ranging [stretching] is the only thing that we know will make changes to joints … the muscle length … splinting will maintain it, but ranging will actually increase muscle length,” Emily said.
Four OTs used orthoses during the day and night because they believed that orthoses reduced spasticity by placing joints in specific spasticity-reducing positions. These OTs used UEOs more often during the day and placed the fingers and wrist in specific positions to immediately reduce spasticity. Zoey said that in her experience, “…when you extend and abduct the thumb, more tone will release in the rest of the hand.”
Finally, four OTs reported that UEOs helped to maintain joint integrity. As such, they designed UEOs such that the arm/hand was in a resting position (slight finger flexion and wrist extension) to maintain natural length of muscles and tendons: “… [with spasticity] the [joints] stay over-stretched or compressed in the position that is not a natural position, so the splint will help to regain balance for all the structures of the hand,” Lily said.
Spasticity severity and range of motion are important client factors guiding UEO implementation
Several factors influenced decision to recommend a UEO (Table 1), with spasticity severity and range of motion most frequently reported by OTs.
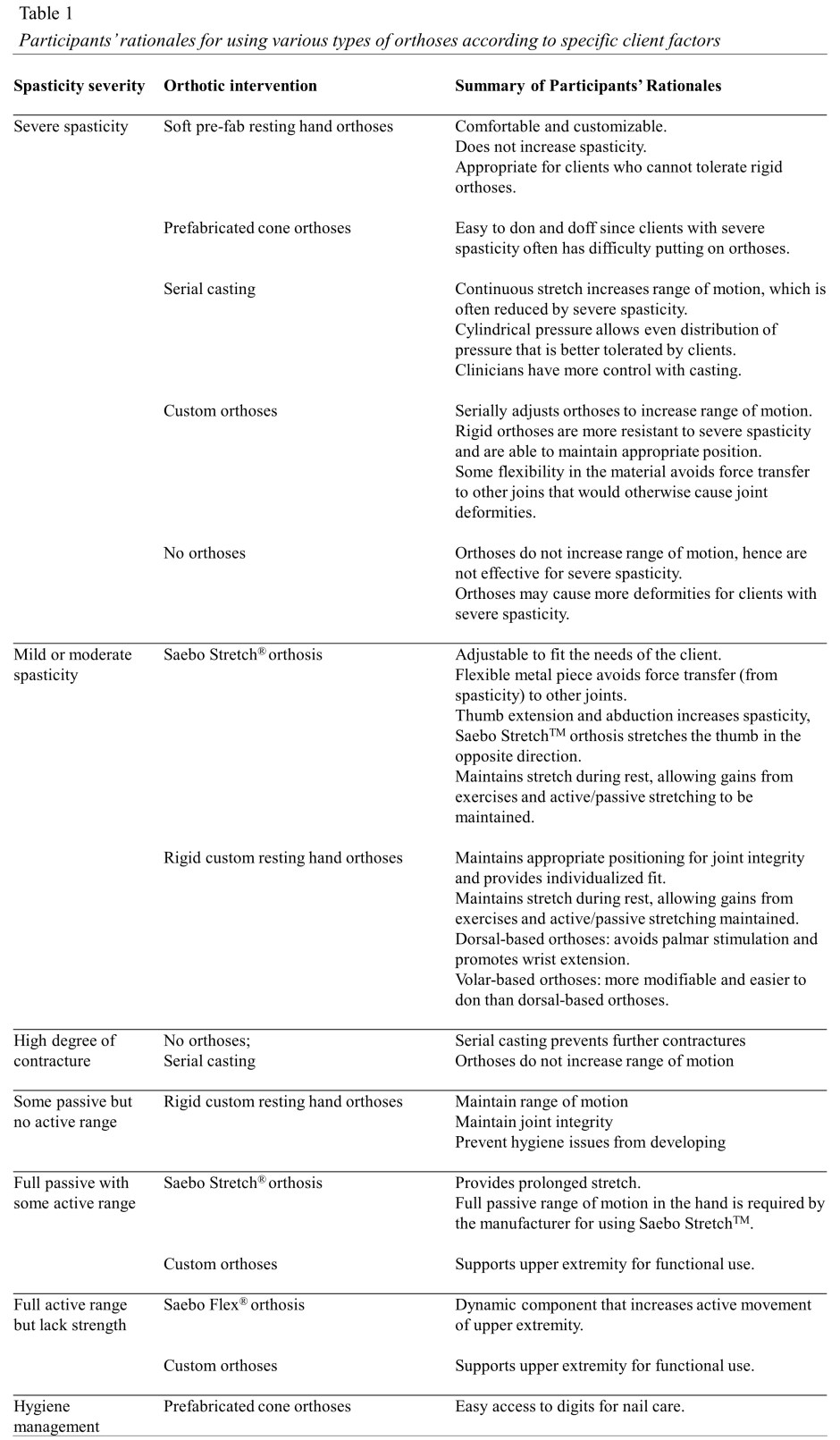
Most OTs, such as Lucas, explained that they often recommended UEOs if their clients were losing range of motion in their joints: “First of all, if they are starting to lose range, and are not able to maintain it, I would definitely try to use a splint,” he said. If the client continued to lose range of motion, more invasive measures such as serial casting (i.e. lightweight fiberglass casts) were also considered.
For clients with severe spasticity, the rationale for using serial casting versus a custom UEO differed among the OTs. Two OTs preferred to use serial casting for severe spasticity because the rigidity of the fiberglass material provided strong resistance to the spasticity while constantly stretching the affected tissues. In contrast, three OTs preferred to use custom-made UEOs, made from softer thermoplastic materials, because it prevented the muscle resistance from spasticity from deforming finger joints, thereby preventing muscle imbalance and joint malalignment.
Valuing clinical experience
Some OTs acknowledged that although the scientific evidence to support orthotic management of spasticity is lacking, they continued to use orthoses because they observed functional changes in their clients. Some of the participants also critiqued the quality of research evidence for spasticity management.
“I know the research doesn’t really show that doing passive range of motion, or splinting [is effective]; there isn’t anything that’s really out there saying, this is really great stuff.”
– Abigail, OT
Given the dearth of research in this area, OTs trust their clinical experience to support their choice to use UEOs. For example, Zoey said: “There’s a lack of research in the custom splints area. For me though, I like to take my first-hand knowledge as well, in addition to reading [the literature].” Participants also identified library resources and continuing education courses as sources of knowledge that guide their practice.
Discussion
These results suggest that OTs’ decisions to use UEOs is guided by their clinical assumptions, client’s spasticity severity, client’s available range of motion, and the OTs’ clinical experience. We identified three assumptions which guided the OTs’ decision-making about UEOs, which were (a) UEOs do not impact spasticity, (b) UEOs can directly reduce spasticity, and (c) UEOs maintain joint integrity, including muscle length. These assumptions represent three different frames of reference (i.e. theoretically-based assumptions that inform clinical decisions) (9,12), and serve as the scientific foundation for OT practice (13). The OTs alluded to, but did not directly discuss three frames of reference: neurophysiology, biomechanics, and neuroplasticity. The former two have been cited in previous literature to explain how UEOs impact spasticity following stroke (5).
From a neurophysiological frame of reference, which focuses on providing interventions to impact aspects of the nervous system, placing joints in specific positions, such as finger abduction, enables the orthosis to directly reduce spasticity, which improves functional use of the arm in daily activities (e.g., bathing, cooking, etc.). A biomechanical frame of reference, which focuses on providing interventions that target biological structures (e.g., muscles, tendons, etc.) assumes that orthoses are used to maintain joint integrity and tissue length and do not have a direct impact on spasticity (5). From a neuroplasticity frame of reference, which focuses on interventions that target motor learning and motor recovery, UEOs may result in unnecessary immobilization of the affected hand. From this perspective, UEOs should be used cautiously and only when necessary (i.e., if the client is losing passive range of motion) (14).
OTs commonly draw on several frames of reference in their intervention with one client but, may eventually select one frame of reference over others as treatment progresses to meet clients’ needs (13). This is well-aligned with the findings in the present report, as the OTs interviewed here stated they begin their intervention plan focusing on motor learning (neurophysiological frame of reference), and then switch the focus to biological structures (biomechanical frame of reference) if the client is losing range of motion.
Considering the lack of high-quality empirical research, OTs use their professional knowledge and clinical experience to guide their decisions. These OTs were aware of their preference to depend on clinical experience, and often chose to disregard the inconsistent research evidence. Though other studies have echoed the significance of clinical experience on OTs’ empirical research utilization in stroke rehabilitation (15), our findings shed new light on their significance in making decisions with UEOs.
Conclusions
There is no single, ideal method for designing and recommending UEOs to manage spasticity. OTs assess and treat based on several client factors, including range of motion and spasticity severity. They also use multiple frames of reference when using UEOs to manage post-stroke spasticity. Given the importance of spasticity severity and range of motion described in this study, future studies that evaluate the effectiveness of UEOs may consider controlling for these factors to enhance the usefulness and utility of future intervention research. More research is needed to explore the effectiveness of UEOs on spasticity, and perhaps, to examine the validity of the theoretical assumptions that are currently guiding OT practice in spasticity management.
References
- Thibaut A, Chatelle C, Ziegler E, Bruno MA, Laureys S, Gosseries O. Spasticity after stroke: Physiology, assessment and treatment. Brain Injury. 2013; 27(10): 1093-105. doi: 10.3109/02699052.2013.804202.
- Duncan P, Zorowitz R, Bates B, et al. Management of adult stroke rehabilitation Care: A clinical practice guideline. Stroke. 2005; 36(9): 100-143. doi: 10.1161/01.STR.0000180861.54180.FF.
- Lannin NA, Herbert RD. Is hand splinting effective for adults following stroke? A systematic review and methodological critique of published research. Clinical Rehabilitation. 2003; 17(8): 807–816. doi: 10.1191/0269215503cr682oa.
- Tyson S, Kent R. The effect of upper limb orthotics after stroke: A systematic review. NeuroRehabilitation. 2011; 28(1): 29-36. doi: 10.3233/NRE-2011-0629.
- Lannin NA, Ada L. Neurorehabilitaion splinting: Theory and principles of clinical use. NeuroRehabilitation. 2011; 28(1): 21–28. doi: 10.3233/NRE-2011-0628.
- Lannin NA, Cusick A, McCluskey A, Herbert RD. Effects of splinting of wrist contracture after stroke: A randomized controlled trial. Stroke. 2007; 38(1): 111-116. doi: 10.1161/01.STR.0000251722.77088.12.
- Harvey L, de Jong I, Goehl G, Mardwedel S. Twelve weeks of nightly stretch does not reduce thumb web-space contractures in people with a neurological condition: a randomized controlled trial. Australian Journal of Physiotherapy. 2006; 52(4): 251–258. doi: 10.1016/S0004-9514(06)70004-6.
- Pizzi A, Carlucci G, Falsini C, Verdesca S, Grippo A. Application of a volar static splint in poststroke spasticity of the upper limb. Archives in Physical Medical Rehabilitation. 2005; 86(9): 1855-1859. doi: 10.1016/j.apmr.2005.03.032.
- Schell BA, Cervero RM. Clinical reasoning in occupational therapy: An interative review. American Journal of Occupational therapy. 1993; 47(7) : 605-610. doi: 10.5014/ajot.47.7.605.
- Sandelowski M. What’s in a name? Qualitative description revisited. Research in Nursing & Health. 2010; 33(1): 77-84. doi: 10.1002/nur.20362.
- Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006; 3(2): 77-101. doi: 10.1191/1478088706qp063oa.
- Dirette DP. Letter from the editor: The importance of Frames of Reference. The Open Journal of Occupational Therapy. 2013; 1(2): 1-6. doi: 10.15453/2168-6408.1039.
- Craik J, Davis D, Polatajko HJ. Introducing the Canadian Practice Process Framework (CPPF): Amplifying the context. In Townsend EA and Polatajko HJ (eds) Enabling Occupation II: Advancing an occupational therapy vision for health, well-being, & justice through occupation. Ottawa, ON: CAOT Publications ACE; 2007: 229-246.
- Sunderland A, Tuke A. Neuroplasticity, learning and recovery after stroke: A critical evaluation of constraint-induced therapy. Neuropsychological Rehabilitation. 2005; 15(2): 81-96. doi: 10.1080/09602010443000047.
- Caldwell E, Whitehead M, Fleming J, Moes L. Evidence-based practice in everyday clinical practice: Strategies for change in a tertiary occupational therapy department. Australian Occupational Therapy Journal. 2008; 55(2): 79-84. doi: 10.1111/j.1440-1630.2007.00669.x.
