
ORIGINAL RESEARCH
By Heather Logan & Gabriela Constantinescu
Introduction
Cancer of the mouth or throat, sometimes referred to as head and neck cancer (HNC), is a devastating disease estimated to affect more than 4,700 Canadians each year (1). Treatment for HNC can include surgery, radiation therapy, and chemotherapy, all of which may cause eating problems. Existing evidence indicates that two thirds of these patients will continue to experience eating difficulties post-treatment. These difficulties can result in medical complications (e.g., malnutrition, dehydration, aspiration pneumonia, or death) and social isolation (2). In some cases, traditional therapies fall short of providing patients with safe and dignified eating and can negatively affect quality of life. For more information about how HNC is assessed and treated, check out “What Science is Doing for Swallowing Problems,” a recent article published in University of Toronto’s Medicine Magazine, along with the work from Starmer, Cousins, McCabe, and their respective colleagues (3-5).
Specialized eating utensils can improve nutrition for HNC survivors, yet few products have been developed and/or are commercially available. This article describes how a specialized eating utensil, known as a glossectomy spoon, was designed through a collaborative partnership between a speech-language pathologist, industrial designers, and a HNC survivor*.
Mary (pseudonym), the HNC survivor, received treatment for a large tumor of the right lower jaw and mouth. She underwent partial glossectomy. This refers to the surgical removal of part of the tongue. Mary’s mouth and tongue was then reconstructed to restore function and appearance. This surgical intervention was followed by radiation and chemotherapy. Mary was later diagnosed with another tumor requiring additional surgeries, which left her with significant eating impairments. Mary estimated that at this time approximately 90 per cent of her nutrition was taken via a feeding tube rather than by mouth.
The primary reason for use of a feeding tube was due to Mary’s severely restricted tongue range of motion and reduced mouth opening. These impairments resulted in substantial effort for Mary to place food at the back of her mouth and swallow. Mary received swallowing therapy to address the strength of the remaining tongue muscles and coordination of her swallow, but even after therapy, she could not safely or comfortably use regular utensils to eat.
Mary addressed this limitation by using a spoon intended for toddlers (i.e., long handle and small bowl). These features allowed Mary to place food further back in her mouth, as well as to rotate the spoon, without scraping the roof of her mouth. While the spoon offered more functional features, Mary was uncomfortable using a spoon designed for toddlers in public. She would avoid eating at social events or she would not attend them. From a rehabilitative perspective, it was important to explore other options and find creative solutions to assist Mary.
The design team aimed to help Mary by designing a spoon that she could comfortably use to eat at social events. To do so, they began by reviewing previous research evidence and applying rehabilitation principles. But only nine scientific articles had been published about adaptive eating utensils or commercially available products for patients, such as Mary, with unique and serious eating difficulties. While few options were described in the literature, experts in the field suggested that any adaptive utensil should be visually appealing and/or not bring attention to the user (6).
The limited options consisted of existing tools adapted for feeding (e.g., syringe) or specialized eating utensils sold at a significant cost (i.e., $256.00 USD) (6-9). Other eating utensils referenced in the literature included some that were no longer commercially available, such as a semi-solid feeder (an injection device that allows the patient to place the food on the back of the tongue) and a glossectomy spoon (10). At the time this study was carried out, the “pusher” spoon (11) and the Glossectomy Placement Feeding Spoon were available for purchase. These two spoons were designed to carry food as far back into the mouth as possible to aid with swallowing. Patients have found both these spoons difficult to use, however, since the size and positioning of the spoons make it challenging to push food into the mouth (12).
Although the current evidence was limited, it informed the design process and choices. So, armed with this evidence, the design team aimed to create an eating utensil for Mary that (a) allowed for easy placement of food in the back of the mouth, (b) contributed to a pleasurable experience while eating, (c) was fabricated out of an appropriate material for the patient, and (d) met material requirements for food safety.
Collaboration and design process
The design team, which included a speech-language pathologist, an industrial designer, and four industrial design students, wanted to develop an eating utensil specific to Mary’s needs and preferences. To do this, the team collaborated with Mary by using her lived experience, treatment history, and feedback.
The first step in the design process was to compile a list of existing spoon designs for patients with and without feeding difficulties. Each spoon design was analyzed based on form, function, materials, manufacturing, and how humans might interact with it (i.e., use it).
Next, Mary’s perspectives were collected through a semi-structured interview and written questionnaire developed by the design team. The purpose of the interview was to better understand the specific eating issues Mary experienced. The questionnaire focused on usability, aesthetics, and design. It was used to prioritize Mary’s needs, wants, and expectations of a specialized spoon.
Interview and idea development
In addition to the information collected through the interview (Table 1) and questionnaire, the design team also observed Mary eating different food consistencies using the toddler spoon.

The information collected in stage one was then used to guide the first prototyping. The industrial designers created numerous sketches (Figure 1) and 3D images (Figure 2) of specialized spoon concepts. Based on Mary’s needs, handle design, spoon bowl size and depth, usability, and visual appearance were all considered in this idea development phase (Figure 3).

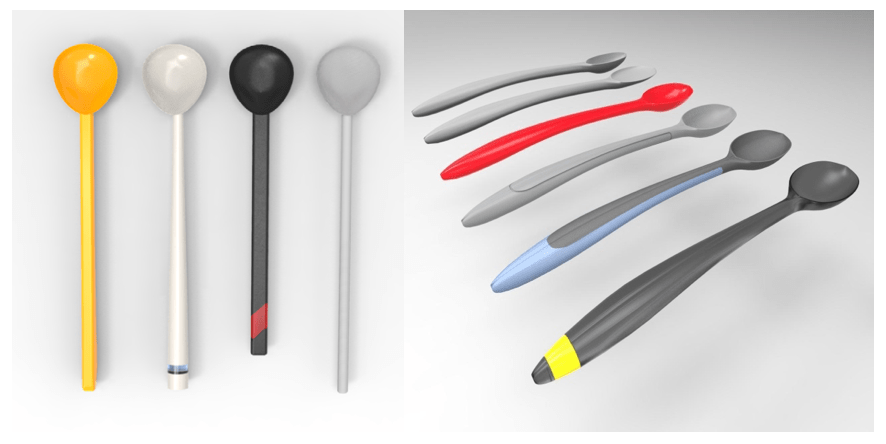
color, handle thickness, and bowl of spoon size and depth.

Design concepts
After reviewing all designs, the team selected six concepts to prototype. The designers modeled these six concepts using Computer-Aided Design (CAD) software and manufactured the models through 3D printing.
The six 3D printed concepts, along with the spoon sketches and photorealistic images, were presented to Mary for feedback. Mary provided the design team with further insight into how she held the spoon and twisted the spoon in her mouth. She also gave important feedback about the handle dimensions and depth of the spoon bowl. Mary chose two of the six concepts that she felt met her functional needs and visual preferences. These two concepts were then developed further based on Mary’s input.
The two final design concepts were 3D printed and prepared to present to Mary once again. Of the two final designs, design concept one was simpler, finding a balance between design and function (Figure 4).
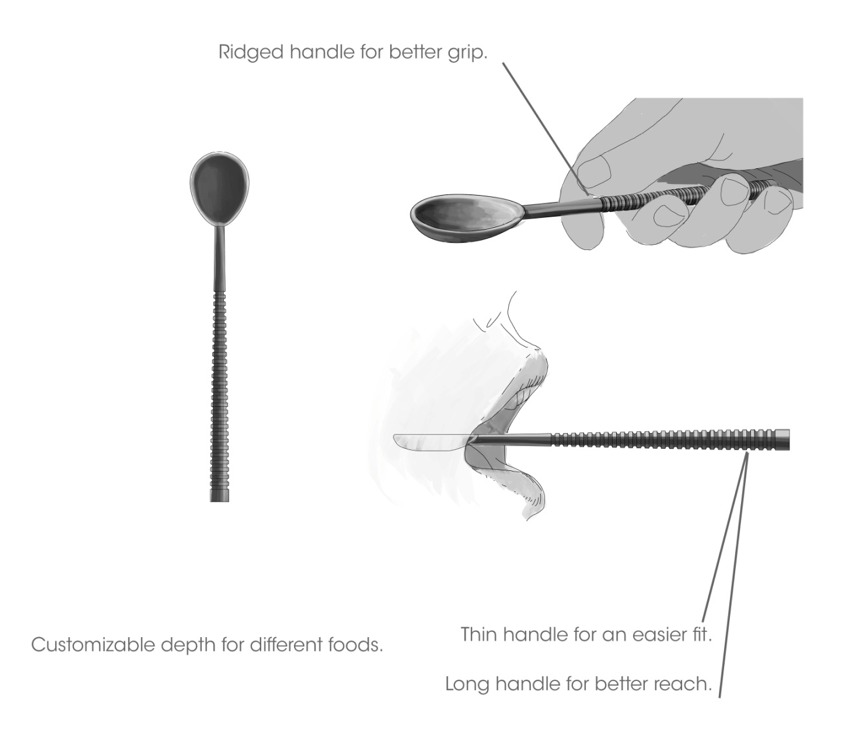
Design concept two considered how user experience could be integrated into a functional everyday object (Figure 5). The handle was designed to comfortably fit in the user’s hand. Three main functionalities were also built into the spoon. First, the maximum distance that the spoon could be inserted into the mouth of this particular individual was clearly marked with a ridge on the handle. This meant that Mary was aware of correct spoon placement without having to sense the bowl on the roof of her mouth. Second, a travel clip feature was added to the bottom of the spoon handle to allow for easy storage within Mary’s pocket. The third feature was the index finger clip to stabilize the utensil during eating.
Mary provided positive feedback on both designs, but ultimately the second design was chosen (Figure 5). Mary preferred the form and function of the second spoon and particularly enjoyed the finger clip feature. She reported that it helped her hold and turn the spoon in her mouth. At this stage, the concept of interchangeable spoon bowls was also explored with Mary. These would allow her to carry different spoon-bowl sizes that could be fitted onto one spoon (rather than carrying multiple spoons) (Figure 6).

Once the various 3D print samples were completed, the design team completed a final interview with Mary. Mary provided feedback on the appearance and the feel of the spoon in her hand. Assessing functionality was limited as the designs were not made of food safe materials. While 3D printing was considered an innovative way to create personalized spoons for patients, they are not yet Food and Drug Administration (FDA) or Health Canada certified as food safe. Some of the other functionalities that Mary was able to trial, such as the finger clasp and the traveler clip, accomplished their desired functionality and were well received. Most importantly, the spoon was visually appealing from the perspective of Mary and the design team. The contemporary appearance of the spoon design was unlike any medical or infant feeding device that is currently available.

Future direction and conclusion
The collaborative design process outlined in this article demonstrates how patient engagement, rehabilitation and design principles, and research evidence can lead to an innovative and functional design to help treat the eating complications experienced by a HNC survivor. In the future, this design and others could be explored with a larger group of participants. Further research and development is also needed to identify a cost-effective way to manufacture a relatively small number of spoons in a food-safe material. For example, manufacturing methods, such as milling and injection molding, could be explored for this purpose. Finally, the impact of this eating utensil on function (e.g., swallow safety and time needed to finish a meal) should be evaluated by additional HNC survivors affected by similar eating impairments.
The collaborative partnership between design and speech-language pathologist experts provided an outcome well beyond the reach of either discipline alone. Nonconventional interdisciplinary collaborations, such as the one described in this article, can bring creative solutions to solving existing clinical dilemma. The outcomes of this particular study created a strong case for design expertise to be used in clinical research and development to improve patient care.
*Mary (pseudonym), the HNC survivor, provided informed consent to participate in the design process and for publication of this article.
Acknowledgments
The authors would like to thank Arthur Hobden, Ivan Au, Stephanie Yong, and Adam Nunn for their contributions during the design process. The authors would also like to thank Mary for her time, support, and valuable feedback. We are also grateful to Dr. Jana Rieger for her valued advice.
References
- Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA: A Cancer Journal for Clinicians. 2017;67(1):7-30.
- Langerman A, MacCracken E, Kasza K, Haraf DJ, Vokes EE, Stenson KM. Aspiration in Chemoradiated Patients With Head and Neck Cancer. Archives of Otolaryngology–Head & Neck Surgery. 2007;133(12):1289-1295.
- Hashem W, Abdelkader R, Abdelkader L, Elhadary S, Mashhour K. PO-117: Swallowing exercises: Will it really help head and neck cancer patients? Radiotherapy and Oncology. 2017;122:56.
- McCabe D, Ashford J, Wheeler-Hegland K, Frymark T, Mullen R, Musson N, et al. Evidence-based systematic review: Oropharyngeal dysphagia behavioral treatments. Part IV–impact of dysphagia treatment on individuals’ postcancer treatments. Journal of Rehabilitation Research and Development. 2009;46(2):205.
- Cousins N, MacAulay F, Lang H, MacGillivray S, Wells M. A systematic review of interventions for eating and drinking problems following treatment for head and neck cancer suggests a need to look beyond swallowing and trismus. Oral Oncology. 2012;49(5):387-400.
- Knott, J.K., Lewin, J.S. Dysphagia Rehabilitation Following Total Glossectomy. Perspectives on Swallowing and Swallowing Disorders (Dysphagia). 2013;22(2):73-80.
- Altschuler, Sheery L., Pidcoe, Susan I., Moss, Bernice B. Oral eating device for food placement. American Journal of Occupational Therapy. 1975;29(4): 229.
- Fleming SM, Weaver AW. Feeding device for glossectomy patients. Archives of Physical Medicine and Rehabilitation. 1983;64(4):183.
- Trible WM. The Rehabilitation of Deglutition Following Head and Neck Surgery. Trible: Dysphagia in Head and Neck Surgery. 1967:518-523.
- Cleary L. An Occupational Therapy Program for Patients With Swallowing Dysfunction Following Cancer Treatment. Occupational Therapy in Health Care. 1986;3(2):23-37.
- Ballard JL, Kerner E, Tyson J, Ashford J, Rees R. Adenocarcinoma of the tongue complicated by a hemimandibulectomy: Soft tissue support for a tongue prosthesis in an edentulous glossectomy patient. The Journal of Prosthetic Dentistry. 1986;56(4):470-473.
- Jensen CB, Evans DL. Swallowing problems in patients with head and neck cancer. Occupational Therapy in Health Care. 1986;3(2):49-62.
